

BronzeSpartan2
Iron
- Joined
- Sep 4, 2023
- Posts
- 130
- Reputation
- 102
I’ve got a hamza tier eye area i know it’s over for me but i want to try looksmaxx anyway. What surgeries can help with this other than orbital decompression (might consider this at last resort) and supraorbital implants and infras?
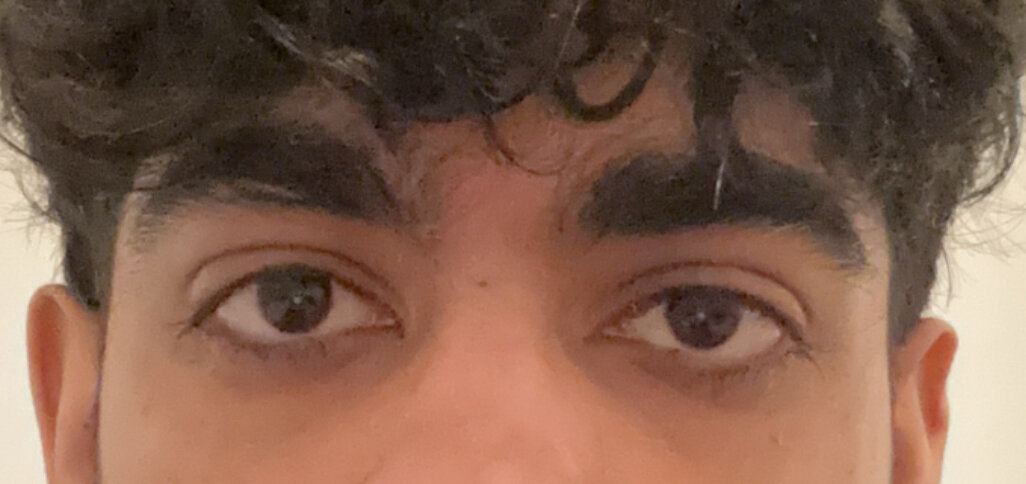
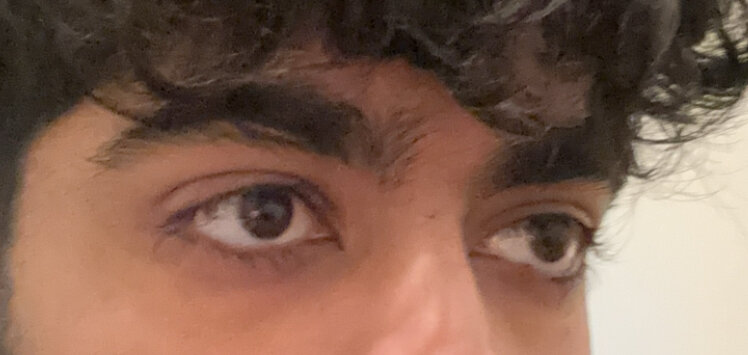

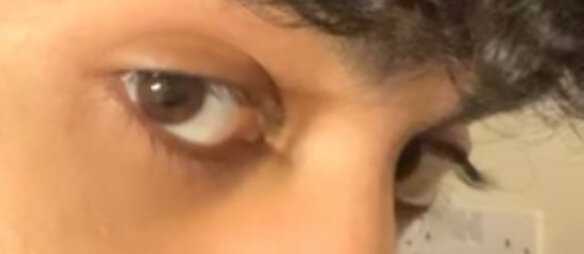

 . I have 60-61Ipd and midface length of 64 and esr of 0.428 but recovery is stil qutie brutal if get 2mm ipd increase doubt it will change alot. I will probably have ideal esr 0.44+ and mid face ratio 0.95+ . But as it been seen some people with low esr does look cyclops because of midfaceratio >0.90 ,eyebrows and icd. So real impact might be less than actual ratios
. I have 60-61Ipd and midface length of 64 and esr of 0.428 but recovery is stil qutie brutal if get 2mm ipd increase doubt it will change alot. I will probably have ideal esr 0.44+ and mid face ratio 0.95+ . But as it been seen some people with low esr does look cyclops because of midfaceratio >0.90 ,eyebrows and icd. So real impact might be less than actual ratios