retard
rides a short bus to school
- Joined
- Apr 6, 2019
- Posts
- 2,699
- Reputation
- 7,990
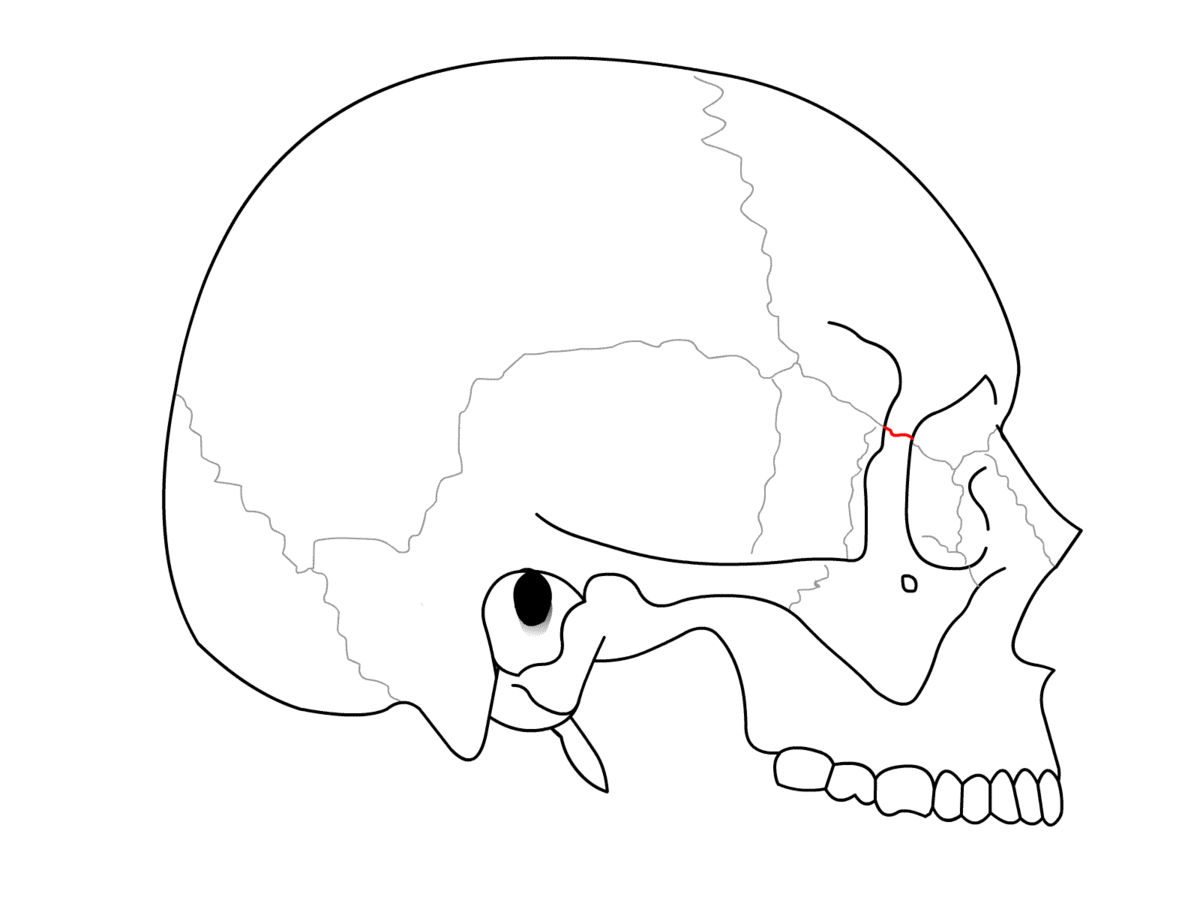
When MSE splits the suture all the force is going to be applied to the bottom of the maxilla, this means that the force is not centralized and that the maxilla will not just be translated outwards, but also rotated, the bottom of the maxilla will be pushed out much more than the top of the maxilla, which is part of the orbital that would cause an increase in IPD

The blue vertical lines is the split maxilla while the arrow is mse splitting the suture and pushing the maxilla out at the bottom, the top red line is the IPD, while the bottom red line is the bizygo distance, notice how when you push the maxilla apart from the bottom the upper maxilla/orbitals move apart minimally in comparison
This is why despite the maxilla/bizygo expanding by 5-6 mm, IPD only expands 1-2mm while you would initially think that since the orbitals are just a part of the maxilla if the maxilla expands 5 mm, the IPD should also increase by 5mm, however this is not the case due to the location that the force is applied
theoretically if you could drill mse in the middle of the maxilla and expanded, the force on it would be centralized resulting in pure translation with no rotations, meaning that the bizygo distance and IPD would increase at a 1:1 ratio
The blue vertical lines is the split maxilla while the arrow is mse splitting the suture and pushing the maxilla out at the bottom, the top red line is the IPD, while the bottom red line is the bizygo distance, notice how when you push the maxilla apart from the bottom the upper maxilla/orbitals move apart minimally in comparison
This is why despite the maxilla/bizygo expanding by 5-6 mm, IPD only expands 1-2mm while you would initially think that since the orbitals are just a part of the maxilla if the maxilla expands 5 mm, the IPD should also increase by 5mm, however this is not the case due to the location that the force is applied
theoretically if you could drill mse in the middle of the maxilla and expanded, the force on it would be centralized resulting in pure translation with no rotations, meaning that the bizygo distance and IPD would increase at a 1:1 ratio