NNBFOIDSLAYER
Iron
- Joined
- Apr 28, 2026
- Posts
- 105
- Reputation
- 59
After dozens of hours researching extraction vs non-extraction outcomes, airway orthodontics, MARPE/MSE literature, orthognathic surgery planning, and cephalometric analysis, I’m making this detailed thread. I just turned 18 and was treated with conventional orthodontics that heavily prioritized dental alignment over facial harmony and airway function. The result is significant midface flattening, transverse maxillary deficiency, poor tongue posture, and chronic nasal breathing impairment. Being severly depressed i decided to make this thread
i will be posting everything: journals, before/after records, analysis, and my current plan. looking for high-quality input from people experienced wit retraction damage recovery / people that have done research on this
Starting Situation
Treatment Executed
Standard extraction camouflage protocol:
Current Situation
while dental alignment and occlusion are now excellent (straight teeth, Class I), the skeletal and soft tissue effects are pretty clear
 )
)
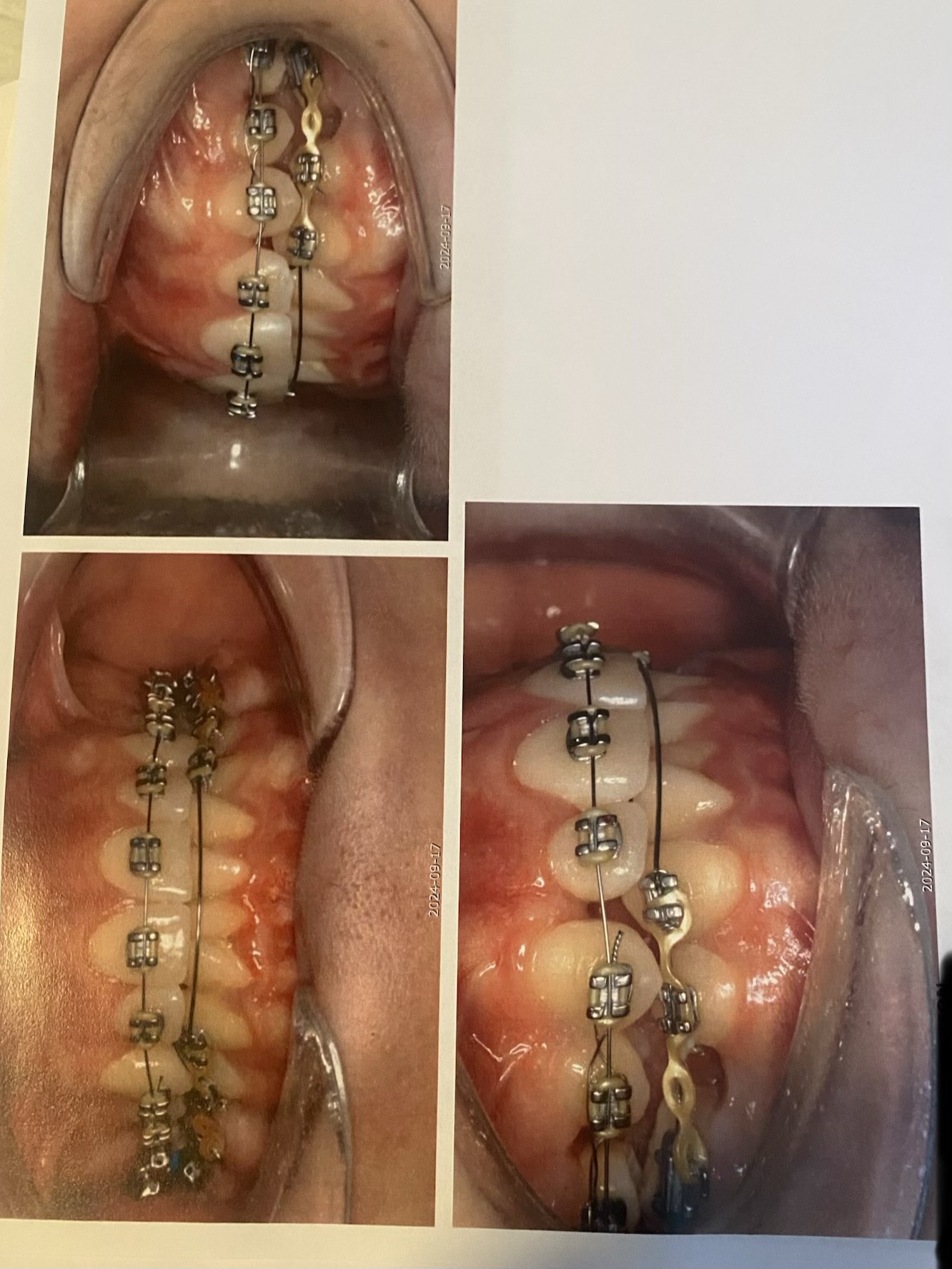
Photos






They noted the "svagt konvext" profile from the beginning but still chose to extract and retract hard. No airway talk, no expansion, just heavy retraction to close spaces
My Analysis
The ortho followed standard traditional protocol for crowding + protrusion: create space via extractions and retract the anterior segent to improve incisor inclination and bite. However, on a patient with already mildly retrusive maxilla, this led to excessive posterior displacement of the maxillary complex. This reduced midface projection (A-point, subnaale, upper lip), constricted the nasal floor, and eliminated proper tongue space
The result is exactly what many researchers in airway and forward growth orthodontics warn about - loss of facial support and compromised respiratory function
Recovery Plan
Phase 1 - Transverse Correction /next 3–6 months
MARPE or MSE-style to achieve skeletal widening
Goals: Increase maxillary width, restore tongue posture, expand nasal cavity volum, improve nasal breathing
Phase 2 - Reassessment
New CBCT, cephalometrics, and clinical evaluation post-expansion stabilization
Considering facemask / reverse-pull headgear for limited sagittal protraction (efficacy most likely limited at 18 but worth attempting)
Phase 3 - Sagitta Correction / likely Necessary
Questions
 I’ll update this thread with new scans when I get them. Appreciate anyone who actually reads all this and gives real input
I’ll update this thread with new scans when I get them. Appreciate anyone who actually reads all this and gives real input
If you want more pictures or have specific questions and is genuinely interested / want better pictures - add me on Discord: _bimaxhopeful_
This took time making and researching trying to fix what they did. Support would be helpful!
i will be posting everything: journals, before/after records, analysis, and my current plan. looking for high-quality input from people experienced wit retraction damage recovery / people that have done research on this
Starting Situation
- Moderate dental crowding with anterior protrusion.
- Neutral anteroposterior relationship (Class I) but with crossbite tendencies (25/35) and minor anterior open bite elements.
- profile: "Svagt konvext" (mildly convex / slightly retrusive maxilla).
- Gummy smile with competent lips.
- Narrow maxillary transverse dimension implied by crowding and arch form.
- overall: Borderline skeletal pattern that could have benefited from expansion rather than extraction camouflage.
Treatment Executed
Standard extraction camouflage protocol:
- Extraction of upper and lower first premolars (15, 25, 35, 45).
- Fixed appliances with heavy retraction mechanics: lacebacks on canines, open coil springs for space maintenance, power chains for anterior retraction, and progressive archwire sequencing (HANT, NiTi, stainless steel).
- Multiple bracket failures and rebonds due to heavy forces.
- Significant anterior retraction to close extraction spaces and achieve ideal overjet/overbite.
- Treatment duration: ~18-24 months.
Current Situation
while dental alignment and occlusion are now excellent (straight teeth, Class I), the skeletal and soft tissue effects are pretty clear
- Maxillary dentoalveolar retraction: posterior displacement of the upper anterior segment, reduced a-point projection, and massive loss of upper lip support
- Transverse maxillary deficiency: Narrow palate persists - inadequate tongue space (tongue rests low, cuts on lower fixed retainer)
- Airway compromise: Reduced nasal cavity volume (maxilla is the floor of the nose), chronic mouth breathing, poor nasal airflow
- Soft tissue profile: shift from mildly convex toward concave appearance, especially subnasal and labial regions
)Photos
They noted the "svagt konvext" profile from the beginning but still chose to extract and retract hard. No airway talk, no expansion, just heavy retraction to close spaces
My Analysis
The ortho followed standard traditional protocol for crowding + protrusion: create space via extractions and retract the anterior segent to improve incisor inclination and bite. However, on a patient with already mildly retrusive maxilla, this led to excessive posterior displacement of the maxillary complex. This reduced midface projection (A-point, subnaale, upper lip), constricted the nasal floor, and eliminated proper tongue space
The result is exactly what many researchers in airway and forward growth orthodontics warn about - loss of facial support and compromised respiratory function
Recovery Plan
Phase 1 - Transverse Correction /next 3–6 months
MARPE or MSE-style to achieve skeletal widening
Goals: Increase maxillary width, restore tongue posture, expand nasal cavity volum, improve nasal breathing
Phase 2 - Reassessment
New CBCT, cephalometrics, and clinical evaluation post-expansion stabilization
Considering facemask / reverse-pull headgear for limited sagittal protraction (efficacy most likely limited at 18 but worth attempting)
Phase 3 - Sagitta Correction / likely Necessary
- Orthognathic surgery: Bimaxillary advancement (Le Fort I maxillary advancement ± BSSO mandibular adjustment, possible CCW rotation + genioplasty).
- Goal: Restoreing proper midface projection, lip support, airway dimensions, and facial harmony
Questions
- Anyone here did MARPE at 18-19 after extractions? How much skeletal expansion did you get and did breathing improve a lot?
- How realistic is facemask protraction at this age?
- For people who got bimax after retraction cases - how many mm advancement did you need to fix the flat midface?
- Good surgeon recs in Europe, especially for aesthetic advancement?
- What tests should I push for (CBCT airway, sleep study etc.)?
I’ll update this thread with new scans when I get them. Appreciate anyone who actually reads all this and gives real inputIf you want more pictures or have specific questions and is genuinely interested / want better pictures - add me on Discord: _bimaxhopeful_
This took time making and researching trying to fix what they did. Support would be helpful!