

Elias
- Joined
- Nov 26, 2019
- Posts
- 7,154
- Reputation
- 15,057
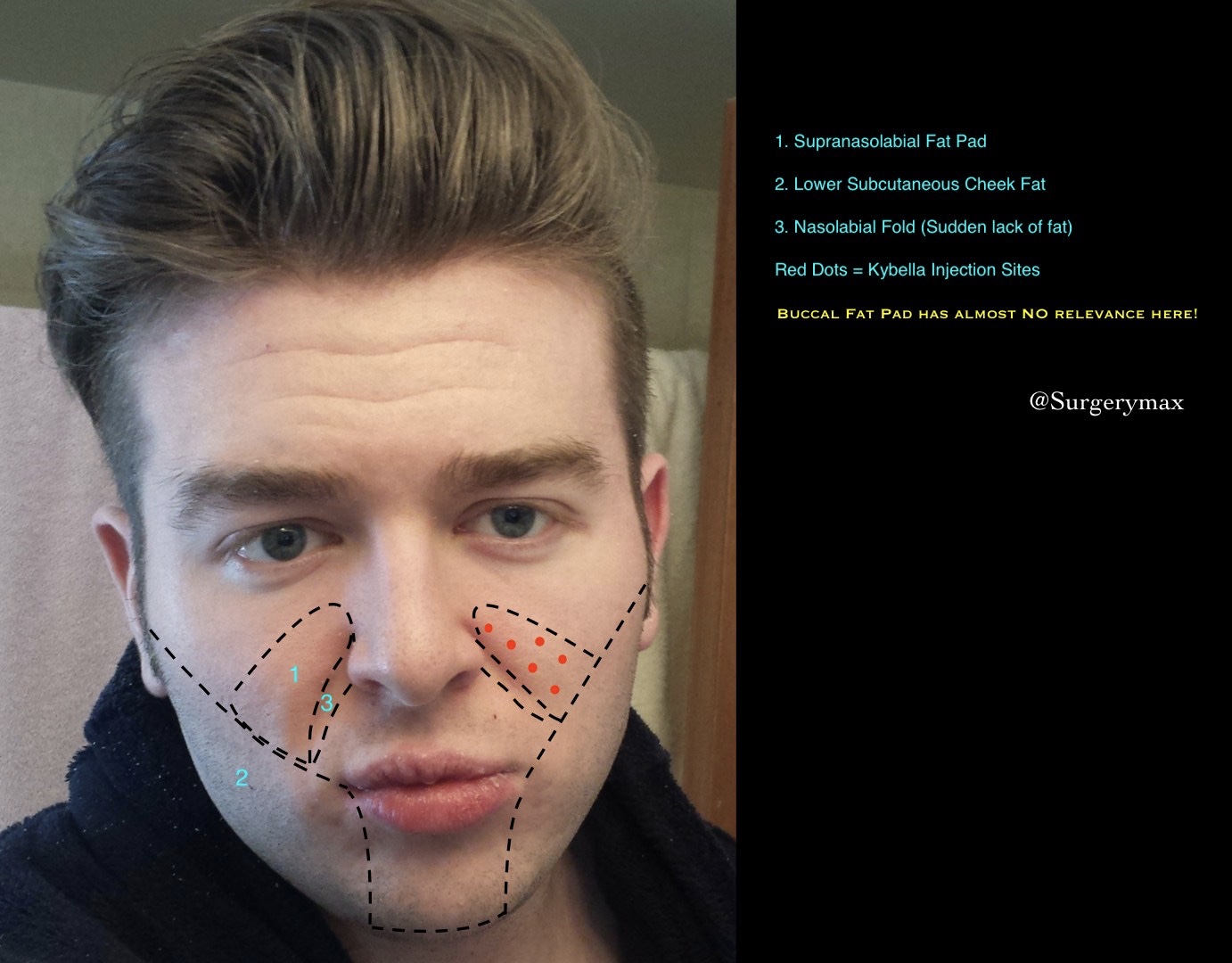
Face fat is almost always thought of incorrectly. First and foremost, it is true that genes and age contribute to resistant fat pads to some extent but this is seldom a total excuse. I will introduce a new defined fat pad: The Supranasolabial Fat Pad and define the region of the Lower Subcutaneous Cheeks. I will also discuss addressing these with Deoxycholic Acid (Kybella) injections as well as Liposuction.
As above, this will be from a clinical perspective and discuss medicine and surgery as an option for management of excessive subcutaneous fat. This article assumes diet & exercise have been exhausted to a full or reasonable extent in its ability to reduce facial fat.
Often the patient presents with concerns of excessive facial fat and are sold the wrong surgical plan. There is an astounding lack of clearly defined regions of facial fat as well as oversimplified theories among plastic surgeons and other aesthetic practicioners. One of these is that fat in the face is a good thing.
I encourage you to take some time studying the anatomical fat distribution of the face in a low body fat individual vs a high (or even average) body fat individual. In the athlete you will notice:
· Nasolabial folds are thin. They exist because of lines in the skin from smiling, rarely because excessive fat hanging or bulging over the nasolabial fold.
· Cheekbones appear more prominent because you can actually see more of them and the bordering area is scooped out because of minimal fat.
“Fat in the face is a good thing” oversimplification
· Minimal subcutaneous fat throughout the face hides the lines and bands created by the muscle. It does not take much fat in the subcutaneous area as the SMAS and platysma muscle lies over skeletal facial muscle, smoothing out the surface.
· While some fat gives youthful volume and realistic contour in the Cheeks, under the Nasolabial folds, and Temples it is unsightly elsewhere in more than minimal amounts.
Defining the Region of Lower Superficial Cheek Fat and the Supranasolabial Fat Pad
Implants and fillers are often erroneously chosen to give the face more definition when selectively removing fat would yield a far more realistic and superior aesthetic result.
· Excessive fat is often the root cause for the lack of bone definition in the face and should be addressed as such.
· Off-setting the lost definition by adding excessive augmentation to normal bones in an overweight face is the wrong approach and will make the face look even more bloated.
· Sometimes instead of adding to an already sufficient area, taking away from the bordering area will scoop it out and make it appear more prominent, a concept proven in BBL surgery.
Why the cheeks have to be liposuctioned or injected with Kybella
· When someone’s face looks doughy, its because what's on the surface – the superficial, subcutaneous fat layer. Not a deeper fat pad which lives under facial muscles (referring to buccal fat pad.)
· Beautiful people have a faint line (and shadow under this line) from approximately the middle of the ear to the corner of the lip. While most notice this – they are trying to achieve this totally by implants or fillers to augment the mid-facial area and not by addressing facial fat.
Why the Supranasolabial Fat Pad needs to be addressed, in relation to cheekbones
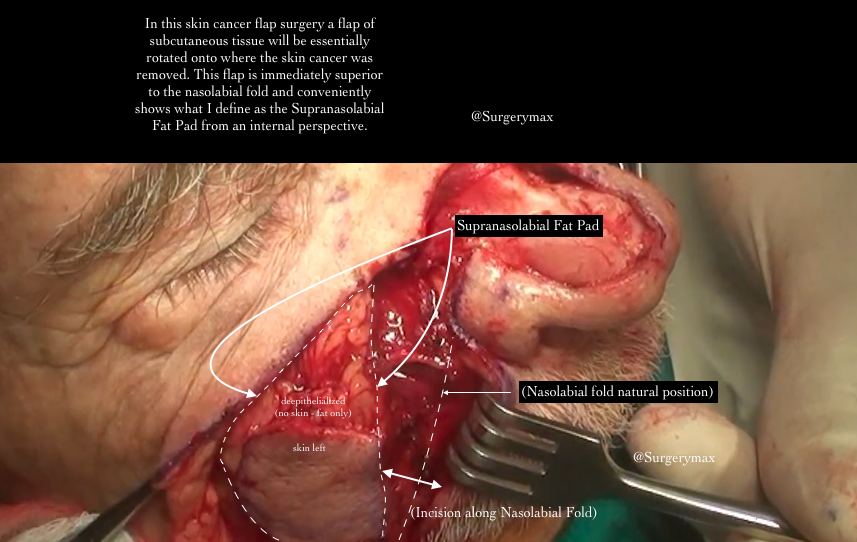
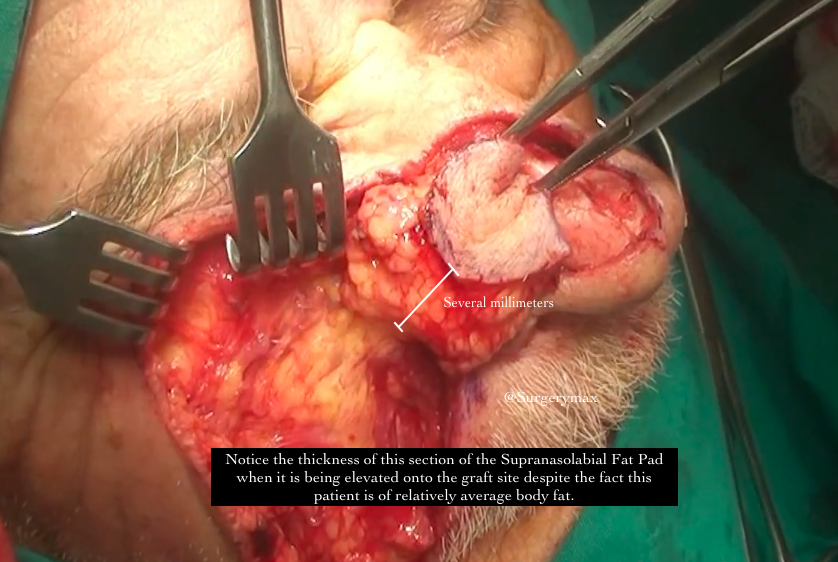
· Excessive fat in the Supranasolabial Pad dwarfs the cheekbones and worsens nasolabial folds. Nasolabial folds are often from a loss of fat in that are but also because of an accumulation of fat causing a sudden rise in the superior border of a nasolabial fold. Adding fat (or fillers) to the nasolabial fold is only one half of an approach which addresses nasolabial folds totally and realistically.
· Liposuctioning the lower back/flanks of a person automatically give the illusion of a more prominent buttock before even injecting any fat into the gluteal region. There are two parts of highlighting the buttock: Injecting fat into the buttock, and Liposuctioning above the buttock. This combination works synergistically to delivery a night and day difference. Addressing the fat around facial bone prominences have the exact same effect.
· Often the cheeks are over-augmented and the nasolabial folds and tear troughs are overfilled to offset the ‘height’ of this fat mound. Augmenting and filling more conservatively, combined with removing a conservative amount of this fat delivers a synergistic and more realistic result.

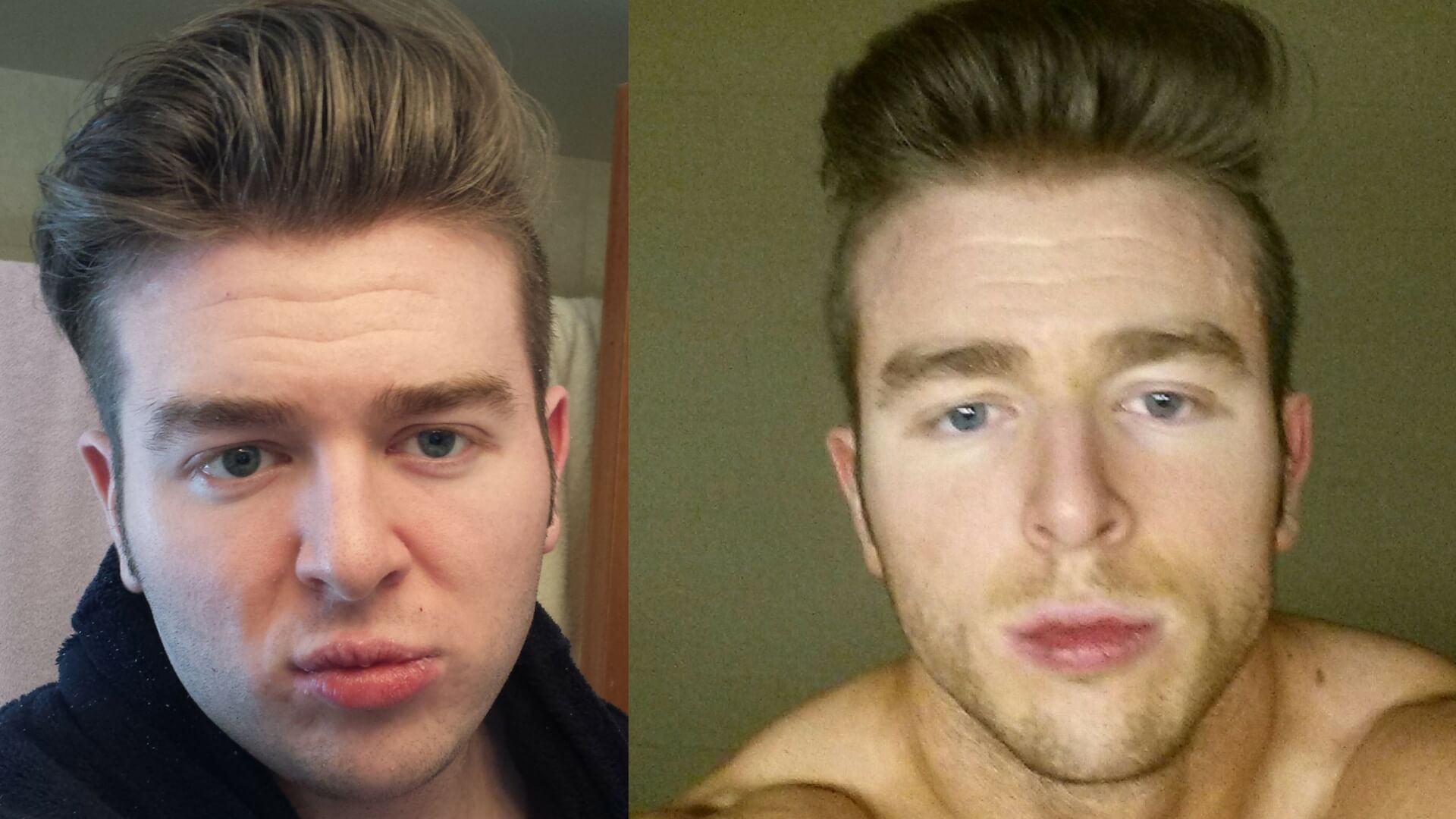
The above subjects lost a considerable amount of bodyfat but underwent no facial bone augmentation.
Why buccal Fat Pad Removal is usually the wrong procedure.
· Buccal fat pad removal is usually underwhelming.
· This deep fat pad layer should usually be preserved as this Deep fat contributes to youthful volume in the cheeks (and a skelator look which is regretted later in life.)
· This surgery requires entering a deeper plane of the face which risks muscles, nerves, and blood vessels more than liposuction or Kybella injections to the subcutaneous plane only.
Why most surgeons do not do liposuction or lipodissolvent injections in the face even though they can.
Many surgeons are simply afraid of contour irregularities or nerve/vascular injury. Further they do not possess the knowledge of "where to draw the line" or recognize defined regions of the face where fat detracts from aesthetic. One very legitmate contraindication is when patients are >30 years old or otherwise have poor skin elasticity. In these populations the removal of fat alone risks saggy skin which is equally if not more unsightly. Of course skin can be excised with a face lift or modified face lift, as well as a rarely done but simple direct excision of the nasolabial fold (with the scar hidden in the natural groove of the nasolabial line.)
However -
· Plastic surgeons actually liposuction the face all the time during a facelift procedure to pre-dissect.
· The entire subcutaneous flap of the face is regularly dissected completely off the underlying structure and SMAS is cut and resected during facelift with little incidence of facial nerve or blood vessel injury, of course liposuction is blind which should be taken into consideration.
· All delicate anatomy (Muscles, Vessels, Nerves, and Glands) live below the SMAS and Platysma.
· Some surgeons offer true cheek liposuction as a standalone procedure with very good results.
· I have seen the Supranasolabial fold liposuctioned before however this would not be my choice.
Kybella on the face??
Yes you can get Kybella injections into the subcutaneous fat in the face above the mandible. Kybella is only approved for a small area under the chin and is technically not even supposed to be injected in the lateral submentum below the ramus per the prescribing information (the white packet that comes with it.) Many practitioners deviate from this but are still reluctant to go above the mandible.
There are five considerations that need to be taken when injecting above the mandible:
1.) Bruising and swelling of the treated area will be far more noticeable and harder to hide.
2.) Loss of fat in the face in populations >30 may not have sufficient skin elasticity and cause sagging
3.) This fat layer is often thinner so it may diffuse farther
4.) Risk of accidental injection into the wrong plane. This can be avoided by asking the patient to clench their facial muscles then pinching the loose subcutaneous fat.
5a.) Defining the areas that get Deoxycholic acid and the ones that do not - This can be hard for some people to put their finger on and relies on a great deal of aesthetic theory. The submental area is clearly defined by the mandible and most people accept this theory however more subtle regions of excessive fat are not readily defined in the literature.
5b.) These areas are defined in a thread I am posting soon about management of face fat.
Per the prescribing information you are not supposed to dilute Kybella but I recommend a concentration of 5-6mg/mL (~ 0.5% or just above) when using above the mandible to lessen skin irritation, and make the process more gradual as very very small amounts of fat lost on the face make a big difference and we don't want to risk taking too much.
For reference, Kybella comes at a concentration of 10mg/mL in the vial or 1%
Correct approaches to True Subcutaneous Cheek Liposuction DO NOT lead to contour irregularities.
Seromas (track left by the liposuction cannula) are from
1. Surgeon using too big of a cannula
2. Burns left by excessive Laser or Ultrasound (Vaser®)
3. Poor technique (It is imperative that the the surgeon spends a lot of time hydro-dissecting, pre-tunneling, and separating the fat evenly before liposuction. Further it is imperative he take a fat equalization step at the end of the procedure preferably using Power Assisted device)
4. Patients disregard post-op instructions – compression and massage. If the Swiss-cheese holes made by the cannula aren’t compressed, they will swell up with fluid and heal with scar tissue inside of them. Patients must FULLY comply with these instructions or the work of their surgeon will be undone and will be a false poor reflection on the surgeon's work.
A proven safe technique for nay-sayers, some modifcations from Dr Klein himself.
*NOT A GUIDE FOR DIY LIPOSUCTION*:
· Separation is not just infiltration – after infiltration about 10-15 minutes on each side should be spent meticulously with a small cannula preferably power assisted without any suction.
· Infiltration needs to be done very meticulously as well. The fluid needs to be distributed evenly throughout the fat and not in pools. Initially using in infiltration cannula can often cause pockets where the fluid goes and is then pushed out when you continue to inject more tumescent solution. It is best to use a 25-gauge spinal needle initially so it has nowhere to go except to swell the extracellular matrix.
· If infiltrated and separated well, the fat will come out with a syringe technique. A wall suction unit or power aspirator should not be used. A syringe allows accurate measurement of exactly what came out on each side as well as low pressure vacuum so it does not tear the SMAS or take fat directly off the underlying skin.
· It does not take much to create a profound difference. As they say “Millimeters are miles on the face” “Milliliters are pints.” (It doesn’t have a nice ring to it but they aren’t exactly liters either...)
Kybella or Liposuction?
Liposuction of the Lower Subcutaneous Cheeks still has risks like liposuction of any other body area. Kybella is not without risk either, and has just as much swelling and sorness as small-cannula liposuction. Liposuction gives an immediate result while Kybella may have to be repeated atleast once and sometimes twice or thrice. Three rounds will mean about 4-5 months before seeing your final result.
In thinner or especially fibrotic patients it may be difficult to liposuction their facial subcutaneous area evenly, and Kybella would be recommended. In these patients too thin for liposuction, one or two rounds will be sufficient.
Kybella is probably always better for the Supranasolabial Fat Pad.
As above, this will be from a clinical perspective and discuss medicine and surgery as an option for management of excessive subcutaneous fat. This article assumes diet & exercise have been exhausted to a full or reasonable extent in its ability to reduce facial fat.
Often the patient presents with concerns of excessive facial fat and are sold the wrong surgical plan. There is an astounding lack of clearly defined regions of facial fat as well as oversimplified theories among plastic surgeons and other aesthetic practicioners. One of these is that fat in the face is a good thing.
I encourage you to take some time studying the anatomical fat distribution of the face in a low body fat individual vs a high (or even average) body fat individual. In the athlete you will notice:
· Nasolabial folds are thin. They exist because of lines in the skin from smiling, rarely because excessive fat hanging or bulging over the nasolabial fold.
· Cheekbones appear more prominent because you can actually see more of them and the bordering area is scooped out because of minimal fat.
“Fat in the face is a good thing” oversimplification
· Minimal subcutaneous fat throughout the face hides the lines and bands created by the muscle. It does not take much fat in the subcutaneous area as the SMAS and platysma muscle lies over skeletal facial muscle, smoothing out the surface.
· While some fat gives youthful volume and realistic contour in the Cheeks, under the Nasolabial folds, and Temples it is unsightly elsewhere in more than minimal amounts.
Defining the Region of Lower Superficial Cheek Fat and the Supranasolabial Fat Pad
Implants and fillers are often erroneously chosen to give the face more definition when selectively removing fat would yield a far more realistic and superior aesthetic result.
· Excessive fat is often the root cause for the lack of bone definition in the face and should be addressed as such.
· Off-setting the lost definition by adding excessive augmentation to normal bones in an overweight face is the wrong approach and will make the face look even more bloated.
· Sometimes instead of adding to an already sufficient area, taking away from the bordering area will scoop it out and make it appear more prominent, a concept proven in BBL surgery.
Why the cheeks have to be liposuctioned or injected with Kybella
· When someone’s face looks doughy, its because what's on the surface – the superficial, subcutaneous fat layer. Not a deeper fat pad which lives under facial muscles (referring to buccal fat pad.)
· Beautiful people have a faint line (and shadow under this line) from approximately the middle of the ear to the corner of the lip. While most notice this – they are trying to achieve this totally by implants or fillers to augment the mid-facial area and not by addressing facial fat.
Why the Supranasolabial Fat Pad needs to be addressed, in relation to cheekbones
· Excessive fat in the Supranasolabial Pad dwarfs the cheekbones and worsens nasolabial folds. Nasolabial folds are often from a loss of fat in that are but also because of an accumulation of fat causing a sudden rise in the superior border of a nasolabial fold. Adding fat (or fillers) to the nasolabial fold is only one half of an approach which addresses nasolabial folds totally and realistically.
· Liposuctioning the lower back/flanks of a person automatically give the illusion of a more prominent buttock before even injecting any fat into the gluteal region. There are two parts of highlighting the buttock: Injecting fat into the buttock, and Liposuctioning above the buttock. This combination works synergistically to delivery a night and day difference. Addressing the fat around facial bone prominences have the exact same effect.
· Often the cheeks are over-augmented and the nasolabial folds and tear troughs are overfilled to offset the ‘height’ of this fat mound. Augmenting and filling more conservatively, combined with removing a conservative amount of this fat delivers a synergistic and more realistic result.
The above subjects lost a considerable amount of bodyfat but underwent no facial bone augmentation.
Why buccal Fat Pad Removal is usually the wrong procedure.
· Buccal fat pad removal is usually underwhelming.
· This deep fat pad layer should usually be preserved as this Deep fat contributes to youthful volume in the cheeks (and a skelator look which is regretted later in life.)
· This surgery requires entering a deeper plane of the face which risks muscles, nerves, and blood vessels more than liposuction or Kybella injections to the subcutaneous plane only.
Why most surgeons do not do liposuction or lipodissolvent injections in the face even though they can.
Many surgeons are simply afraid of contour irregularities or nerve/vascular injury. Further they do not possess the knowledge of "where to draw the line" or recognize defined regions of the face where fat detracts from aesthetic. One very legitmate contraindication is when patients are >30 years old or otherwise have poor skin elasticity. In these populations the removal of fat alone risks saggy skin which is equally if not more unsightly. Of course skin can be excised with a face lift or modified face lift, as well as a rarely done but simple direct excision of the nasolabial fold (with the scar hidden in the natural groove of the nasolabial line.)
However -
· Plastic surgeons actually liposuction the face all the time during a facelift procedure to pre-dissect.
· The entire subcutaneous flap of the face is regularly dissected completely off the underlying structure and SMAS is cut and resected during facelift with little incidence of facial nerve or blood vessel injury, of course liposuction is blind which should be taken into consideration.
· All delicate anatomy (Muscles, Vessels, Nerves, and Glands) live below the SMAS and Platysma.
· Some surgeons offer true cheek liposuction as a standalone procedure with very good results.
· I have seen the Supranasolabial fold liposuctioned before however this would not be my choice.
Kybella on the face??
Yes you can get Kybella injections into the subcutaneous fat in the face above the mandible. Kybella is only approved for a small area under the chin and is technically not even supposed to be injected in the lateral submentum below the ramus per the prescribing information (the white packet that comes with it.) Many practitioners deviate from this but are still reluctant to go above the mandible.
There are five considerations that need to be taken when injecting above the mandible:
1.) Bruising and swelling of the treated area will be far more noticeable and harder to hide.
2.) Loss of fat in the face in populations >30 may not have sufficient skin elasticity and cause sagging
3.) This fat layer is often thinner so it may diffuse farther
4.) Risk of accidental injection into the wrong plane. This can be avoided by asking the patient to clench their facial muscles then pinching the loose subcutaneous fat.
5a.) Defining the areas that get Deoxycholic acid and the ones that do not - This can be hard for some people to put their finger on and relies on a great deal of aesthetic theory. The submental area is clearly defined by the mandible and most people accept this theory however more subtle regions of excessive fat are not readily defined in the literature.
5b.) These areas are defined in a thread I am posting soon about management of face fat.
Per the prescribing information you are not supposed to dilute Kybella but I recommend a concentration of 5-6mg/mL (~ 0.5% or just above) when using above the mandible to lessen skin irritation, and make the process more gradual as very very small amounts of fat lost on the face make a big difference and we don't want to risk taking too much.
For reference, Kybella comes at a concentration of 10mg/mL in the vial or 1%
Correct approaches to True Subcutaneous Cheek Liposuction DO NOT lead to contour irregularities.
Seromas (track left by the liposuction cannula) are from
1. Surgeon using too big of a cannula
2. Burns left by excessive Laser or Ultrasound (Vaser®)
3. Poor technique (It is imperative that the the surgeon spends a lot of time hydro-dissecting, pre-tunneling, and separating the fat evenly before liposuction. Further it is imperative he take a fat equalization step at the end of the procedure preferably using Power Assisted device)
4. Patients disregard post-op instructions – compression and massage. If the Swiss-cheese holes made by the cannula aren’t compressed, they will swell up with fluid and heal with scar tissue inside of them. Patients must FULLY comply with these instructions or the work of their surgeon will be undone and will be a false poor reflection on the surgeon's work.
A proven safe technique for nay-sayers, some modifcations from Dr Klein himself.
*NOT A GUIDE FOR DIY LIPOSUCTION*:
· Separation is not just infiltration – after infiltration about 10-15 minutes on each side should be spent meticulously with a small cannula preferably power assisted without any suction.
· Infiltration needs to be done very meticulously as well. The fluid needs to be distributed evenly throughout the fat and not in pools. Initially using in infiltration cannula can often cause pockets where the fluid goes and is then pushed out when you continue to inject more tumescent solution. It is best to use a 25-gauge spinal needle initially so it has nowhere to go except to swell the extracellular matrix.
· If infiltrated and separated well, the fat will come out with a syringe technique. A wall suction unit or power aspirator should not be used. A syringe allows accurate measurement of exactly what came out on each side as well as low pressure vacuum so it does not tear the SMAS or take fat directly off the underlying skin.
· It does not take much to create a profound difference. As they say “Millimeters are miles on the face” “Milliliters are pints.” (It doesn’t have a nice ring to it but they aren’t exactly liters either...)
Kybella or Liposuction?
Liposuction of the Lower Subcutaneous Cheeks still has risks like liposuction of any other body area. Kybella is not without risk either, and has just as much swelling and sorness as small-cannula liposuction. Liposuction gives an immediate result while Kybella may have to be repeated atleast once and sometimes twice or thrice. Three rounds will mean about 4-5 months before seeing your final result.
In thinner or especially fibrotic patients it may be difficult to liposuction their facial subcutaneous area evenly, and Kybella would be recommended. In these patients too thin for liposuction, one or two rounds will be sufficient.
Kybella is probably always better for the Supranasolabial Fat Pad.




