Orka

DIY Aesthetician
- Joined
- Sep 8, 2024
- Posts
- 16,456
- Reputation
- 55,327
Hello all, I'd like to start this off by saying this is not a theory made by me, I was talking in a discord server when this was brought to my attention, a person called sasx introduced me to it.
I've been and will be extremely busy for the next few weeks, so I won't have time to fact check, skim or really go through almost any of this, so I wanted to share it here and ask what you guys think.




there are inhibitors of SOST who stimulate bone osteogenesis via b catenin signaling




here it clearly says how wnt signaling impacts bone growth and there’s so many more info on this its common knowledge
also bmp drugs

there are also epigenetic modulators

bone damage does obviously stimulate bone remodeling, and the process of repairing it includes osteogenesis and the bone repairing thicker, ofc the more ur osteoblasts get stimulated the more it is efficient, plus u can do it for long time



pth is literally an injectable hormone, u can take drugs that are legit for any process that includes stimulant bone growth at any age and bone remodeling doesn’t stop w puberty either
and HGH is good to add on cycles it also stimulates osteoblasts via igf1 + its good for sleep, collagen etc
The spoiler above is a copy pasted message from the DM on discord, they refused to share the source of the text.
I'd appreciate comments specifically referring to parts of the theory rather than "nah its cope".
Tagging people who might know something about this:
@aids @chadisbeingmade @SlayerJonas
I'd be willing to pay one of the people above to go through this in depth if its too much to look through in your free time. Thanks!
I've been and will be extremely busy for the next few weeks, so I won't have time to fact check, skim or really go through almost any of this, so I wanted to share it here and ask what you guys think.


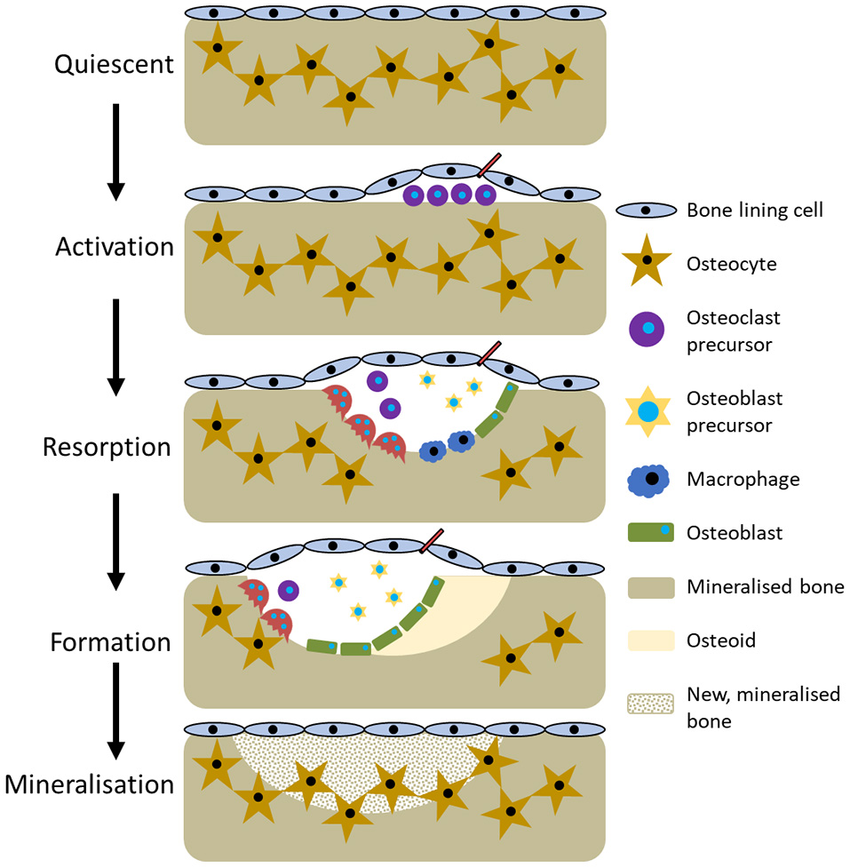
- bone remodeling


there are inhibitors of SOST who stimulate bone osteogenesis via b catenin signaling




here it clearly says how wnt signaling impacts bone growth and there’s so many more info on this its common knowledge
also bmp drugs

there are also epigenetic modulators
- and drugs that heavily stimulate runx2 pathways
- this is also very true u can ask doctors irl aswell

bone damage does obviously stimulate bone remodeling, and the process of repairing it includes osteogenesis and the bone repairing thicker, ofc the more ur osteoblasts get stimulated the more it is efficient, plus u can do it for long time



pth is literally an injectable hormone, u can take drugs that are legit for any process that includes stimulant bone growth at any age and bone remodeling doesn’t stop w puberty either

and HGH is good to add on cycles it also stimulates osteoblasts via igf1 + its good for sleep, collagen etc
The spoiler above is a copy pasted message from the DM on discord, they refused to share the source of the text.
I'd appreciate comments specifically referring to parts of the theory rather than "nah its cope".
Tagging people who might know something about this:
@aids @chadisbeingmade @SlayerJonas
I'd be willing to pay one of the people above to go through this in depth if its too much to look through in your free time. Thanks!