P
pslislaw
Iron
- Joined
- Apr 10, 2026
- Posts
- 32
- Reputation
- 29
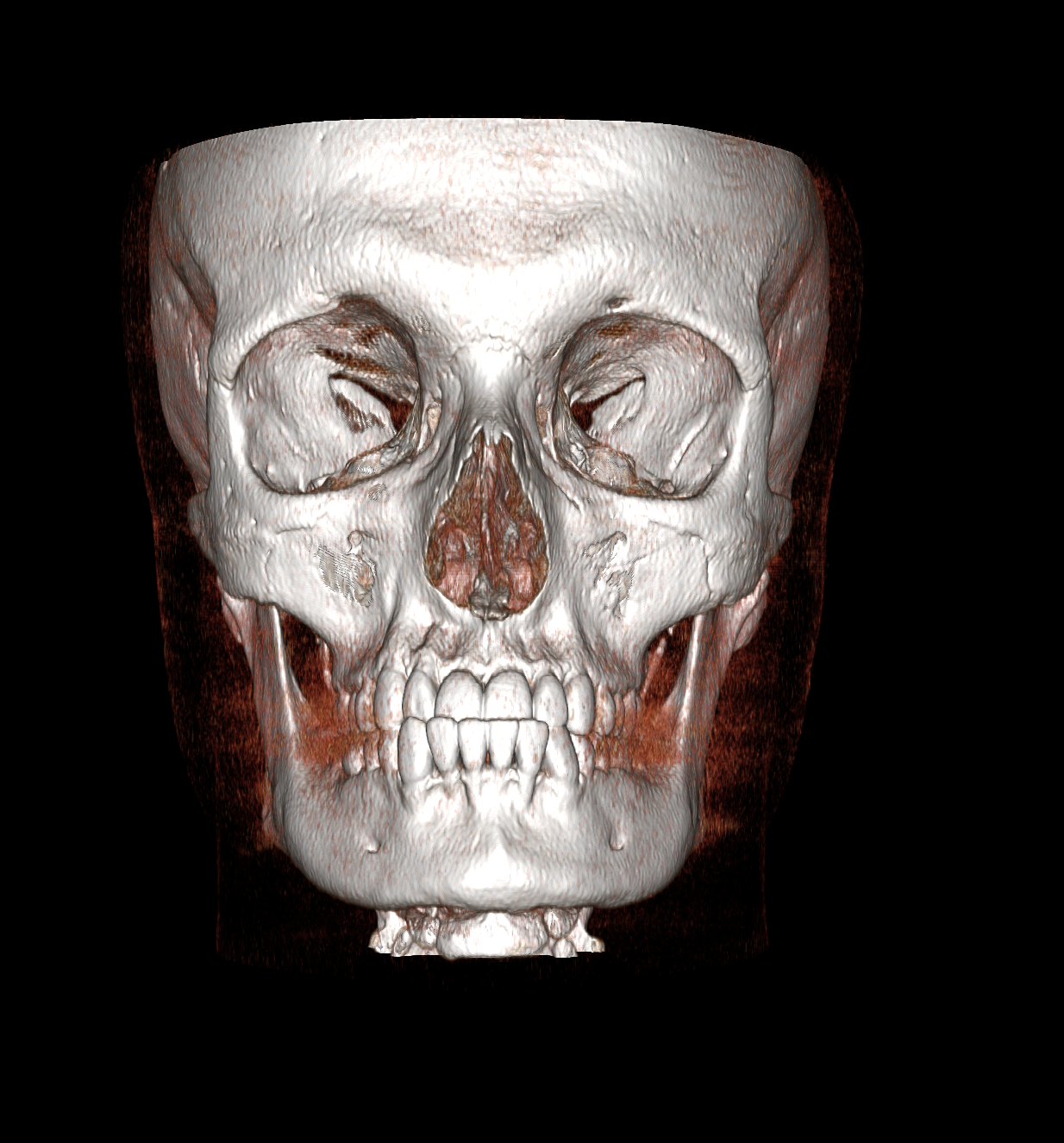
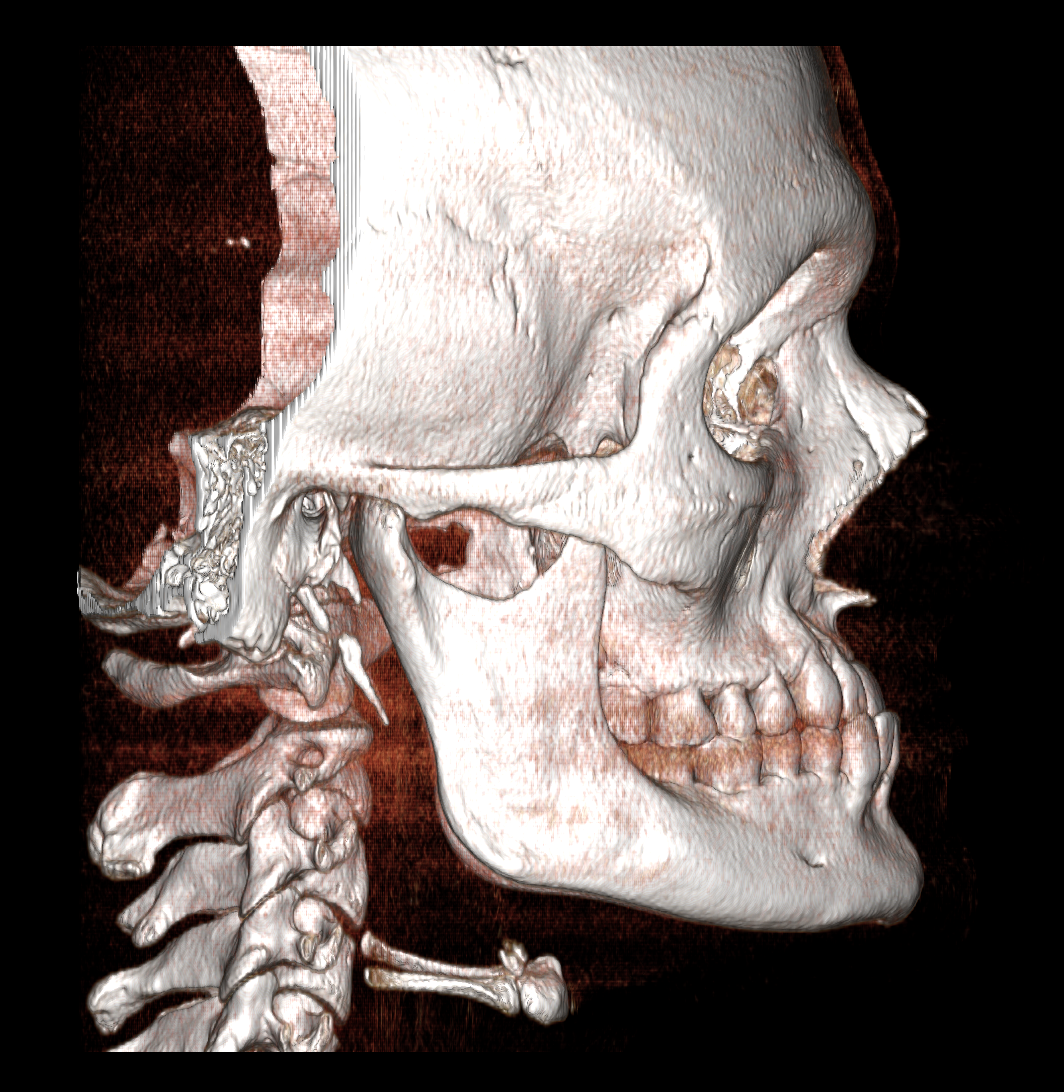
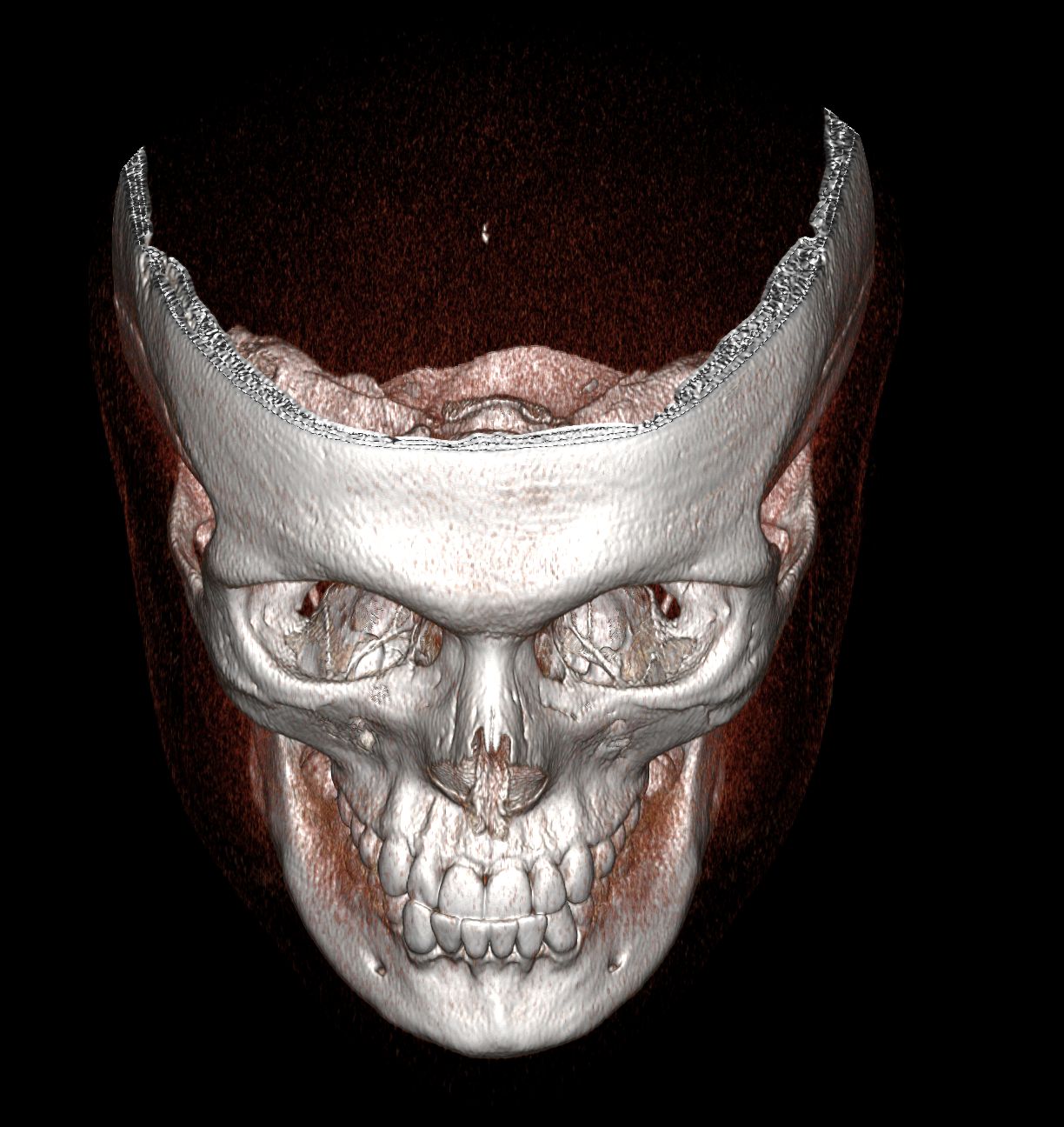
Just got my CT scans done prior to my custom planning for Lefort 1 + BSSO + Genioplasty
I'll post the plan my surgeon does once he's done with the actual 3D planning
Initial notes from my orthodontist (I had braces + tooth-borne palate expander as a kid. I never wore my elastics because I couldn't be fucked but now I'm glad I didn't. LARPed hard to get a referral to the maxfac surgeon who I black-pilled across the course of multiple consults over 1.5 years.):
Dear ___,
Thank you for seeing ___. ___ has been under our care since 2017. He initially presented with a class I
dental malocclusion on a skeletal 3 base with a horizontal pattern of growth. He was treatment planned for RME with fixed
appliances with the potential for extractions in the lower arch.
He commenced with an RME at the end of 2017 and his fixed appliances went on in 2018. Unfortunately, we have struggled
to gain positive overjet, and we have struggled for an excessively long time. There were periods of missed appointments
and Covid lockdown may have contributed to this protracted treatment time. His Class III skeletal growth has worsened
over this time.
We have been asking ___ to use elastics also for an extended period of time and unfortunately recently he has been
experiencing facial / TMJ pain following the use of elastics. He locates the pain to the masseter muscle and there is
significant tenderness on palpation of the left masseter.
He now presents with a concave profile with moderately deficient midface, mild prognathic mandible and horizontal
mandibular plane. Intra orally he presents with class III molar relationship with minimal overbite and overjet (edge to edge
incisal relationship). His lateral ceph shows a retrognathic maxilla and very mild mandibular prognathism. His OPG shows
impacted 8s and his recent opg now shows the presence of an odontome occlusal to the 28 which was not discernable
previously.
We recently reviewed ___'s treatment goals in detail and ___ has expressed that he would like to address his
skeletal discrepancy and facial profile. I also believe that extraction in the lower arch would be detrimental to his
aesthetics.
We would be grateful if you could assess ___ for bimaxillary surgery and possible genioplasty.
Thank you for your help.
Initial notes from my surgeon (this was October 2025, just an initial rough plan):
Surgical Plan:
1. Le Forte I osteotomy with advancement of approximately 7mm and 3mm downward movement
2. Bilateral sagittal split osteotomy (BSSO) advancement
3. Genioplasty with 5mm advancement
Clinical Findings:
The patient presents with deficient maxillary projection and reduced tooth show on smiling. Cephalometric
analysis shows a brachyfacial growth pattern with a relatively flat occlusal plane. The posterior airway space is
notably large at 18mm, approximately in the 90th percentile. There is evidence of nasal congestion, particularly
marked on the left side with enlarged turbinates.
Current Issues:
- Reduced maxillary projection
- Limited tooth show on smiling (requires 4-5mm additional show)
- TMJ clicking without pain or functional limitation, occasional locking
- Impacted wisdom teeth
- Nasal congestion and breathing difficulties
Treatment Discussion:
The surgical movements will include maxillary advancement of 7mm with 3mm downward repositioning to
achieve optimal tooth show. While the mandibular position is technically acceptable, patient preference is for
additional projection through BSSO and genioplasty. The estimated cost for the complete procedure has been
discussed.
My thoughts:
The movements will 100% need to be more aggressive as they are pretty conservative right now. We have discussed this and he is designing the cuts & movements as we speak.
I'll post the plan my surgeon does once he's done with the actual 3D planning
Initial notes from my orthodontist (I had braces + tooth-borne palate expander as a kid. I never wore my elastics because I couldn't be fucked but now I'm glad I didn't. LARPed hard to get a referral to the maxfac surgeon who I black-pilled across the course of multiple consults over 1.5 years.):
Dear ___,
Thank you for seeing ___. ___ has been under our care since 2017. He initially presented with a class I
dental malocclusion on a skeletal 3 base with a horizontal pattern of growth. He was treatment planned for RME with fixed
appliances with the potential for extractions in the lower arch.
He commenced with an RME at the end of 2017 and his fixed appliances went on in 2018. Unfortunately, we have struggled
to gain positive overjet, and we have struggled for an excessively long time. There were periods of missed appointments
and Covid lockdown may have contributed to this protracted treatment time. His Class III skeletal growth has worsened
over this time.
We have been asking ___ to use elastics also for an extended period of time and unfortunately recently he has been
experiencing facial / TMJ pain following the use of elastics. He locates the pain to the masseter muscle and there is
significant tenderness on palpation of the left masseter.
He now presents with a concave profile with moderately deficient midface, mild prognathic mandible and horizontal
mandibular plane. Intra orally he presents with class III molar relationship with minimal overbite and overjet (edge to edge
incisal relationship). His lateral ceph shows a retrognathic maxilla and very mild mandibular prognathism. His OPG shows
impacted 8s and his recent opg now shows the presence of an odontome occlusal to the 28 which was not discernable
previously.
We recently reviewed ___'s treatment goals in detail and ___ has expressed that he would like to address his
skeletal discrepancy and facial profile. I also believe that extraction in the lower arch would be detrimental to his
aesthetics.
We would be grateful if you could assess ___ for bimaxillary surgery and possible genioplasty.
Thank you for your help.
Initial notes from my surgeon (this was October 2025, just an initial rough plan):
Surgical Plan:
1. Le Forte I osteotomy with advancement of approximately 7mm and 3mm downward movement
2. Bilateral sagittal split osteotomy (BSSO) advancement
3. Genioplasty with 5mm advancement
Clinical Findings:
The patient presents with deficient maxillary projection and reduced tooth show on smiling. Cephalometric
analysis shows a brachyfacial growth pattern with a relatively flat occlusal plane. The posterior airway space is
notably large at 18mm, approximately in the 90th percentile. There is evidence of nasal congestion, particularly
marked on the left side with enlarged turbinates.
Current Issues:
- Reduced maxillary projection
- Limited tooth show on smiling (requires 4-5mm additional show)
- TMJ clicking without pain or functional limitation, occasional locking
- Impacted wisdom teeth
- Nasal congestion and breathing difficulties
Treatment Discussion:
The surgical movements will include maxillary advancement of 7mm with 3mm downward repositioning to
achieve optimal tooth show. While the mandibular position is technically acceptable, patient preference is for
additional projection through BSSO and genioplasty. The estimated cost for the complete procedure has been
discussed.
My thoughts:
The movements will 100% need to be more aggressive as they are pretty conservative right now. We have discussed this and he is designing the cuts & movements as we speak.