dookielooksmaxxer
Message for 1 on 1 coaching.
- Joined
- Jul 10, 2024
- Posts
- 873
- Reputation
- 789
You may have known @ihatemySOST for the subperiosteal hematoma thing blah blah blah whatever. Basically, anyone who believed him needs to start thinking about themselves. In this thread I'll simply just expose his retarded arguements.
Subperiosteal Hematoma:
Already debunked him on this: https://looksmax.org/threads/finall...ot-ultra-high-iq-thread.1641470/post-23918842
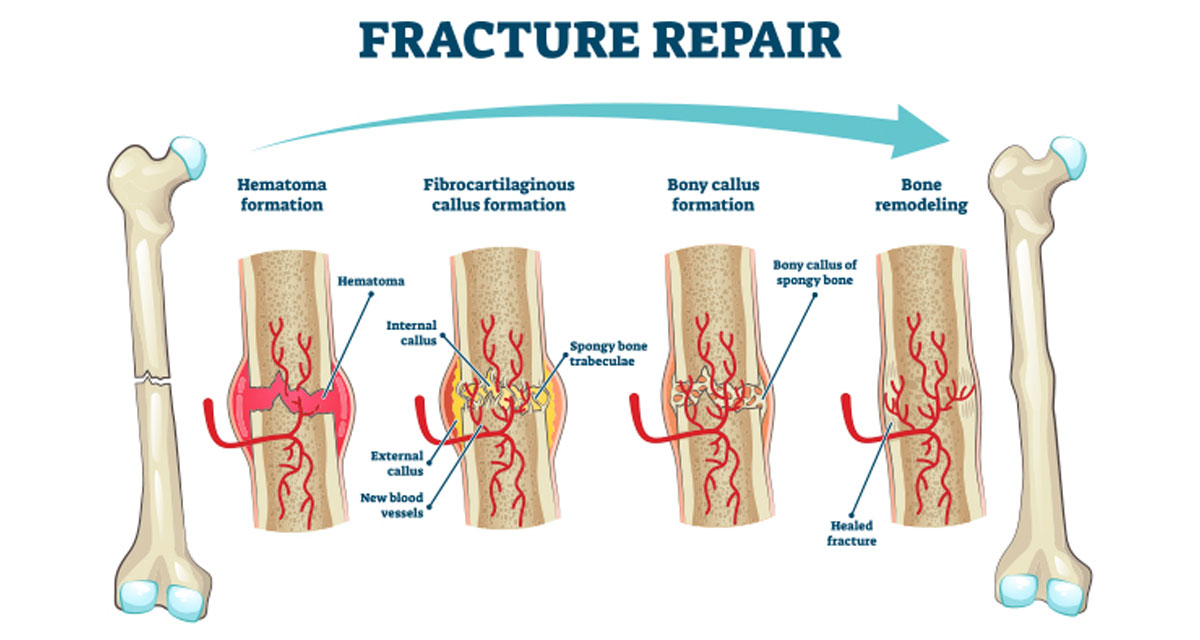
Basically it causes bleeding between the periosteum and bone when traumatic/non-traumatic forces occur. The problem with this, is that it actually isn't proper bone growth. Rather, its a balloon of blood that could potentially ossify in that balloon form. So basically, your going to look deformed!




He also agreed with me that it won't work for aesthetics aswell LMAO


PTH analogues
Okay so this retard states that its not going to work for both bone mass/jaw growth but only proves his claim for... jaw growth...

I'll still debate both points, however.
On Bone Mass:
Sources:
 pmc.ncbi.nlm.nih.gov
pmc.ncbi.nlm.nih.gov

 www.sciencedirect.com
www.sciencedirect.com

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov

 www.nejm.org
"In contrast to the antiresorptive agents, anabolic agents can directly stimulate osteoblastic
www.nejm.org
"In contrast to the antiresorptive agents, anabolic agents can directly stimulate osteoblastic
formation of new bone. The only anabolic agent currently FDA-approved in the United
States is parathyroid hormone (1-34) (PTH 1-34), or teriparatide"
PTH analogues (such as teriparatide/abaloparatide) are FDA-approved and are generally used in human osteoporosis treatment.

"Treatment of postmenopausal osteoporosis with parathyroid hormone (1-34) decreases the risk of vertebral and nonvertebral fractures; increases vertebral, femoral, and total-body bone mineral density; and is well tolerated"

It's pretty safe to say that in humans, PTH analogues can work for radial bone growth if used correctly. I'll get into how to use it correctly (just briefly, I won't actually provide a guide on it since thats not the point of this thread.)
So it works for radial bone growth, what else should we know??
Not sure if you guys do know, but PTH analogues need to be used PTH analogues intermittently in order to effectively get results, otherwise it will turn catabolic overtime (in other words, it will give diminishing returns or bone resorption.)
The reason is why is quite simple. The R^0 state refers to Prolonged cAMP signaling, which will bias bone resorption rather than bone formation.
On the other hand, the RG state efers to transient cAMP signaling, shifting the bias to bone formation.

This would also prove that abaloparatide is arguably better than teriparatide because of bias towards the RG state.
On Mandibular Growth:


TLDR OF HIS ARGUEMENT: yea bro since rats need alot higher of a dose to get mandibular growth, so do you!!! (I'm ignorant of one factor however, the fact that rat physiology differs from human physiology.)
Sprague-Sawley rats (the same rats he utilized in his study) have a much lower ABL bioavailability after subq administration, which would explain the large dosages used.

(source: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/208743Orig1s000PharmR.pdf)
BUT MUHHH DOOKIELOOKSMAXXER!!!! THEY ARENT THE SAME RAT:

They are the same lab rat strain.
Therefore, for mandibular growth, abaloparatide should work perfectly fine within normal ranges of dosaging and if you use it intermittently. (too lazy to look too deep into that mechanism but it seems to me it would be upregulation of Sox9 in the condyle.)
TLDR
It baffles me how you guys will just believe anything you see on the internet. High iq individuals on org are now classified as people who do research, but they don't need to be right.

Subperiosteal Hematoma:
Already debunked him on this: https://looksmax.org/threads/finall...ot-ultra-high-iq-thread.1641470/post-23918842
Basically it causes bleeding between the periosteum and bone when traumatic/non-traumatic forces occur. The problem with this, is that it actually isn't proper bone growth. Rather, its a balloon of blood that could potentially ossify in that balloon form. So basically, your going to look deformed!
He also agreed with me that it won't work for aesthetics aswell LMAO
PTH analogues
Okay so this retard states that its not going to work for both bone mass/jaw growth but only proves his claim for... jaw growth...
I'll still debate both points, however.
On Bone Mass:
Sources:
Parathyroid Hormone and Parathyroid Hormone-related Protein Analogs as Therapies for Osteoporosis - PMC
Osteoporotic fractures result in significant morbidity and mortality. Anabolic agents reverse the negative skeletal balance that characterizes osteoporosis by stimulating osteoblast-dependent bone formation to a greater degree than ...
pmc.ncbi.nlm.nih.gov
PTH/PTHrP analogues as osteoanabolic treatment in patients with osteoporosis
Teriparatide (TPTD) and abaloparatide (ABL) are osteoanabolic drugs belonging to the group of parathyroid hormone analogues and parathyroid hormone-re…
Molecular properties of the PTH/PTHrP receptor - PubMed
The receptor for parathyroid hormone (PTH) and PTH-related protein (PTHrP) is a G protein-coupled receptor (GPCR) that plays a key role in controlling blood Ca(2+) concentration and endochondral bone formation. This review focuses on the molecular mechanisms by which the receptor recognizes the...
pubmed.ncbi.nlm.nih.gov
Effect of Parathyroid Hormone (1-34) on Fractures and Bone Mineral Density in Postmenopausal Women with Osteoporosis | NEJM
Once-daily injections of parathyroid hormone or its amino-terminal fragments increase bone formation and bone mass without causing hypercalcemia, but their effects on fractures are unknown. We rand...
formation of new bone. The only anabolic agent currently FDA-approved in the United
States is parathyroid hormone (1-34) (PTH 1-34), or teriparatide"
PTH analogues (such as teriparatide/abaloparatide) are FDA-approved and are generally used in human osteoporosis treatment.
"Treatment of postmenopausal osteoporosis with parathyroid hormone (1-34) decreases the risk of vertebral and nonvertebral fractures; increases vertebral, femoral, and total-body bone mineral density; and is well tolerated"
It's pretty safe to say that in humans, PTH analogues can work for radial bone growth if used correctly. I'll get into how to use it correctly (just briefly, I won't actually provide a guide on it since thats not the point of this thread.)
So it works for radial bone growth, what else should we know??
Not sure if you guys do know, but PTH analogues need to be used PTH analogues intermittently in order to effectively get results, otherwise it will turn catabolic overtime (in other words, it will give diminishing returns or bone resorption.)
The reason is why is quite simple. The R^0 state refers to Prolonged cAMP signaling, which will bias bone resorption rather than bone formation.
On the other hand, the RG state efers to transient cAMP signaling, shifting the bias to bone formation.
This would also prove that abaloparatide is arguably better than teriparatide because of bias towards the RG state.
On Mandibular Growth:
TLDR OF HIS ARGUEMENT: yea bro since rats need alot higher of a dose to get mandibular growth, so do you!!! (I'm ignorant of one factor however, the fact that rat physiology differs from human physiology.)
Sprague-Sawley rats (the same rats he utilized in his study) have a much lower ABL bioavailability after subq administration, which would explain the large dosages used.
(source: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/208743Orig1s000PharmR.pdf)
BUT MUHHH DOOKIELOOKSMAXXER!!!! THEY ARENT THE SAME RAT:
They are the same lab rat strain.
Therefore, for mandibular growth, abaloparatide should work perfectly fine within normal ranges of dosaging and if you use it intermittently. (too lazy to look too deep into that mechanism but it seems to me it would be upregulation of Sox9 in the condyle.)
TLDR
It baffles me how you guys will just believe anything you see on the internet. High iq individuals on org are now classified as people who do research, but they don't need to be right.
Attachments

Last edited: