IQMaxxedSubhuman
Iron
- Joined
- Jul 6, 2026
- Posts
- 11
- Reputation
- 19
Thread song:
"Can chewing mastic gum fix this?"
I asked, sliding a candid side-profile photo
across the desk. It highlighted my melting chin, the soft transition from jaw to
throat, and a complete absence of a gonial angle.
One of the top maxillofacial surgeons in the country just laughed, pulled up a
CBCT scan, and showed me exactly why my skull was the actual problem.
Since then, I’ve analyzed hundreds of scans, consulted with world-class
specialists, and helped dozens of guys on this board navigate surgery. I know
what actually works, and I'm tired of watching guys waste their prime on useless
orthotropics.
Here is the brutal truth: most "lower third" guides here are garbage. They are
written by fifteen-year-olds who think chewing hard gum or injecting some
peptides for two weeks will magically swing their mandible forward. It won’t,
JFL. If your skeletal structure is recessed, no amount of mewing is going to
save you once your growth plates are fully fused.
This thread is the definitive blueprint. I am laying out the exact mechanics of
the lower third by age group—because what works for a twelve-year-old with open
sutures will do absolutely nothing for a twenty-five-year-old with a locked
skull.
We are going to dissect:
Section I: The Clinical Baseline — Why Your Mirror Is Lying to You
Stop staring in the bathroom mirror. If you're on this board, you've probably spent hours holding your phone at head-height, tilting your chin up at a 45-degree angle under downlight, trying to convince yourself that your lack of a jawline is just water retention. It’s a massive cope. Mirror frauding doesn't change your skeletal reality.
JFL. If you have to thrust your jaw forward to look normal, you have a structural deficit. Let's look at the actual physics of why you look like a thumb in unposed photos.
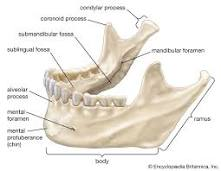
The maxilla is your facial foundation, locked directly into the skull. The mandible is a separate bone suspended by muscles, ligaments, and joints. Your chin is merely a small projection on the front of that mandible—it is not the jaw itself.
Draped over this bone scaffold is your soft tissue: skin, fat pads, the platysma muscle, masseters, and submental tissue. While soft tissue can temporarily camouflage mild skeletal recessions, soft tissue cannot fundamentally change where your bones sit. If your underlying bone framework lacks projection, your soft tissues will sag, bunch up, and melt into your neck. You cannot solve a structural volume deficit with fat-loss or topical tricks.
Vertical growth causes the mandible to swing down and back instead of forward (vertical maxillary excess).

When your mandible is recessed (an SNB below 76°), your tongue and soft palate get shoved back toward your spine, choking your airway. On a lateral ceph, a healthy airway is 10mm to 12mm wide. If yours is choked down to 6mm, you're borderline suffocating.
To keep you breathing, your brain drops your hyoid bone—the free-floating bone anchoring your tongue—down and back to open up the airway.
This drop drags the surrounding soft tissue down with it, creating that sloping, melted neck-to-chin line. You can starve yourself down to 8% body fat, but you'll never get a sharp 90-degree submental angle. The skin can't tighten because the bone scaffold is too far back. Never try to starve away a double chin caused by a recessed mandible; you'll just look emaciated with the exact same soft neck.
If your scans show a steep FMA and a choked airway, your lower third is a skeletal issue. Stop wasting money on face rollers and soft-maxxing copes. The bone has to move. Let's look at how we actually change the skeletal frame.

Trying to widen or advance a fused skull with your tongue or hard gum is a losing battle against basic physics. Your skull is not a soft lump of clay. It is a highly secure system of solid bones locked together by fibrous joints called sutures [2]. As you age, these sutures undergo interdigitation—they twist, mesh, and eventually fuse into solid, unmovable bone (synostosis).

━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Skeletal Expansion vs. Dental Tipping
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━[/CENTER>
Most orthodontists are lazy. When an adult patient has a narrow palate and a crossbite, the orthodontist will often use a standard quad-helix or a rapid palatal expander (RPE) anchored solely to the teeth.
In a grown adult, this does not expand the jawbone. It causes dental tipping.
The Dental Tipping Trap: Why Orthodontists Ruin Faces
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
When teeth are tipped outward to make the dental arch look wider, the roots of the teeth are forced against the thin outer plate of the jawbone (the buccal cortex).
This causes severe structural damage:
• Gingival recession: The gums shrink away from the tilted teeth.
• Bone loss (Dehiscence): The tooth root physically pushes through the bone envelope.
• Unstable occlusion: The moment you take your retainer out, your teeth instantly collapse back inward.
Every single day, my inbox gets trashed with blurry, down-lit side profiles from guys looking for a cheap shortcut. Drunk on TikTok "hormone-maxxing" trends, they genuinely believe a vial of liquid Masteron or a handful of research peptides is going to chemically rescue a recessed lower third and turn them into Chico.
It won't.
Let's look at the actual clinical endocrinology. Your skeleton isn't static rock. It is highly active metabolic tissue. But your ability to remodel that bone is entirely dictated by the biological clock of your secondary cartilages and the site-specific density of your androgen receptors (AR).
The craniofacial complex doesn't react to sex steroids the same way the rest of your body does. A femur or clavicle has a standard baseline of androgen receptors. The mandibular condyle, masseter attachment sites, and the cortical plates of the mandible? They are dense, hyper-reactive hotbeds for AR expression.
In vitro assays of human osteoblastic cells (HOCs) prove this. Cells pulled from the mandible express up to three times the AR mRNA of those taken from the axial skeleton.
This intense, localized receptor density is what actually drives the sexual dimorphism of the male skull. It creates the flared gonial angle, the lateral ramus width, the forward projection of the chin, and the heavy brow ridge. Dihydrotestosterone (DHT) carves out these traits, but it only does so during highly specific developmental windows.
Once your skeletal sutures and cartilaginous zones fuse, the door slams shut.
Before you even think about pinning anything, you need to define what "growing your jaw" means for your specific skull. Fixing a recessed lower third requires manipulating two entirely different vectors of bone growth. Each is governed by different chemical stacks and biological limits.
Stop guessing based on your chronological age. Look at the biological markers.
If you're in this bracket, your long bone epiphyseal plates are basically done. But you have a biological loophole: the secondary cartilage of the mandibular condyle is still metabolically active. This specific cartilage bypasses standard endochondral ossification and responds aggressively to mechanical strain and systemic GH/IGF-1 levels.
Deploying highly androgenic, non-aromatizing compounds alongside recombinant growth hormone (rhGH) during this narrow window forces the condyle to lay down new bone.
The absolute dealbreaker? Estrogen. Estrogen (E2) drives growth plate fusion and condylar mineralization in both sexes. If you run heavily aromatizing cycles—like high-dose testosterone—you will spike your systemic E2, instantly fuse your growth zones, and permanently lock your mandible into its recessed state.
Once you hit 21, the game completely changes. Condylar cartilage? Mineralized. Sutures? Locked. You cannot chemically lengthen your lower third past this point. Period.
Blasting high-dose GH or IGF-1 as an adult won't buy you a single millimeter of forward mandibular length. You're just asking for localized acromegaly. Because the bone can no longer grow longitudinally, the excess GH forces appositional growth. Your skeleton just gets thicker. You walk away with heavy orbital rims, a bloated brow ridge, and massive hands.
The soft-tissue changes are even worse. GH abuse causes macroglossia (tongue expansion). The muscle pushes against your teeth, blowing out massive gaps (diastemas) and forcing your mouth into a flared, "chimp-lip" profile. Your nasal cartilage coarsens. Your skin gets thick and oily. You completely wreck your facial aesthetics.
But adult androgen-driven appositional growth is still highly viable for engineering lateral jaw flare. By targeting the cortical bone of the gonial angles, you can physically widen your lower third.
Let's bury the main DIY forum cope right now: smearing DHT cream (like Andractim) directly on your jawline.
It shows a massive misunderstanding of how transdermal pharmacokinetics and skeletal biology actually work.
If your bones are fused, you missed the pubertal window, and a $20k BSSO/genioplasty is out of the question, you have exactly one non-surgical option left to fix a compressed lower third: Beard Frauding.
By cultivating dense facial hair (using 5% topical Minoxidil and a 1.5mm dermaroller if your genetics are trash), you can visually reconstruct your facial thirds. Keep the cheek lines trimmed tight to preserve zygomatic definition, but let the hair on the chin and jawline grow out. By edging the bottom line a centimeter below your actual mandible and squaring off the chin, you artificially drop your visual lower third. It creates the illusion of a vertically balanced face without touching a single osteoblast.
Between the ages of 13 and 15, your growth plates are highly active and
incredibly responsive—both in the long bones for vertical height and the
mandibular condyles for your jaw. Capitalizing on this peak developmental window
requires maximizing systemic IGF-1 levels. Pharmaceutically, this is done by
running high-purity Recombinant Human Growth Hormone (rhGH) at 2 IU to 3 IU
daily, administered subcutaneously on an empty stomach right before sleep.
Because estrogen (E2) drives epiphyseal plate fusion and limits your growth
runway, keeping estrogen in a low-normal range is non-negotiable if you want to
delay joint mineralization. You can manage this pharmaceutically with a
micro-dose of Anastrozole (0.25 mg once or twice a week). Alternatively, you can
stack natural estrogen modulators. Start with Boron (6 mg daily) to lower SHBG,
which increases free testosterone while naturally lowering serum estradiol. Pair
this with 100 mg of DIM (Diindolylmethane) daily to shift estrogen metabolism
away from the highly active 16-alpha pathway, and add Zinc Picolinate (30 mg
daily) to act as a mild, natural aromatase inhibitor. To maximize endogenous
testosterone, introduce Tongkat Ali (200 mg daily). It stimulates luteinizing
hormone (LH) to boost Leydig cell output without shutting down your developing
HPTA, supplying the precise androgenic signaling your skeleton needs for density
and structural definition.
While systemic hormones provide the raw building blocks, mechanical forces
dictate where that new bone is actually deposited. Proper oral posture (mewing)
is vital to guide the remodeling maxilla upward and forward, preventing a
down-swung, long-face profile. To complement this, introduce progressive
mechanical loading. Chewing hard mastic gum for 20 minutes every other day
triggers mechanotransduction, signaling the mandibular condyle to remodel and
expand at the jaw joints. This dual approach leverages elevated GH and free
testosterone to widen your dental arches and project the lower third forward.
Finally, to fuel this rapid osteogenesis, support the protocol with a targeted
bone-mineralization matrix: 5,000 IU of Vitamin D3 and 5 mg of Vitamin K2 (MK-4)
daily. This specific pairing routes calcium directly into your lengthening
skeletal frame instead of soft tissues, locking in every last millimeter of
potential height and jawline projection.
 𝑻𝒉𝒆 𝑺𝒕𝒆𝒓𝒐𝒊𝒅 𝑻𝒊𝒎𝒊𝒏𝒈 𝑻𝒉𝒆𝒐𝒓𝒚
𝑻𝒉𝒆 𝑺𝒕𝒆𝒓𝒐𝒊𝒅 𝑻𝒊𝒎𝒊𝒏𝒈 𝑻𝒉𝒆𝒐𝒓𝒚
Here is my theory on the
optimal timing for
anabolic steroid use,
specifically for
maximizing overall bone mass
and
optimizing lower-third skeletal development.
To the 1% of you with the focus to actually make it this far: pause. Take a deep, deliberate breath. Walk to your kitchen, pour a glass of ice water, and stand in front of the mirror. Don't scan your reflection for flaws. Look at yourself to recognize the face and body of the person you are actively architecting.
ok back to topic
these are a few options worth checking out:
█ HIGH TIER / FULLY LEGIT[/B>
Verified Peptides
https://verifiedpeptides.com/product/bpc-157-tb-500-blend/
• Category: Peptides (BPC-157, TB-500, GHK-Cu) • Quality: High
(Third-party verified) • Pricing: Standard Retail • Verdict: The
gold standard for domestic peps. If you're prioritizing purity for injury
recovery or skinmaxxing and don't want to gamble with your health, start here.
Deus Power https://deuspower.shop/ •
Category: Androgens, PCT, HGH, SARMs • Quality: Very High
(Authorized Deus Medical reseller) • Pricing: Competitive •
Verdict: Top-tier reliability. Deus is widely regarded as one of the best
EU labs on the forum. Shipping is discreet—usually disguised as vitamins or
cosmetic oils—making them the premier choice for EU/UK buyers.
Driada Medical https://driadashop.to/
• Category: Androgens, HGH, PCT, SARMs • Quality: Very High
(Lab-tested / smooth carrier oils) • Pricing: Standard Retail •
Verdict: A dominant EU-domestic heavyweight that easily rivals Deus. They
are highly praised on Meso-Rx for their strict testing transparency and
exceptionally smooth carrier oils (primarily sesame, keeping PIP non-existent).
Just watch out for fake clone domains (like shopdriada.eu)—only order from the
official .to site.
Steroidify
https://www.steroidify.ltd/Trenbolone
• Category: Androgens, PCT, Ancillaries • Quality: High /
Brand-dependent (Stocks official Deus, Pharmacom, etc.) • Pricing:
Premium • Verdict: The "concierge" option. You're paying a convenience
markup, but the professional customer service, delivery guarantees, and payment
flexibility are unmatched in this space.
─────────────────────────────────────────────────────
█ MID TIER / SITUATIONAL[/B>
TheBBPower https://thebbpower.com/ •
Category: AAS, HGH, PCT • Quality: Solid (Official Hilma Biocare
distributor) • Pricing: Standard UGL • Verdict: A dedicated EU
domestic source heavily pushing Hilma Biocare. Vouched for on MesoRX as a
reliable European option, but proceed with caution—enough scattered complaints
exist regarding slow shipping and dropped communications on secondary boards to
warrant a test order first. Viable, but Deus Power remains the superior EU
route.
Iron Lion Lab
https://ironlion-lab.is/shop/ •
Category: HGH, Peptides, AAS • Quality: Reliable (Well-reviewed
across major boards) • Pricing: Extremely Cheap (Lowest cost-per-IU on
HGH) • Verdict: The budget king for heightmaxxing runs via Puretropin.
The gear is solid, but shipping can be an absolute nightmare. Order weeks in
advance or prepare to wait.
UK-Peptides
https://www.uk-peptides.com/ •
Category: Peptides • Quality: Consistent • Pricing:
Standard • Verdict: The safest bet for UK/EU buyers who want fast
shipping and zero customs anxiety.
AllDayChemist
https://www.alldaychemist.com/ •
Category: Prescription Drugs (Accutane, Aromasin, Hair Loss, PCT) •
Quality: Pharma-Grade (Generic Indian pharma) • Pricing: Cheap •
Verdict: An industry veteran. The go-to for cheap Accutane, Finasteride,
or Dutasteride. While the purity is pharmaceutical standard, be prepared for a
clunky payment process and shipping that takes weeks.
─────────────────────────────────────────────────────
█ OVERPRICED / AVOID[/B>
MisteRoid Pharma
https://misteroidpharma.site/shop/
• Category: AAS / Underground Lab • Quality: Highly Suspect
(Unverified / Shilled) • Pricing: Honeypot • Verdict: Hard pass.
Major red flags across the board. Forum veterans recently exposed their rep on
Eroids for allegedly spinning up dummy accounts to spam five-star reviews on
their own gear. Don't risk injecting unverified bathtub oil when established,
top-tier labs are readily available.
Enhanced Labs
https://enhancedlabs.com/collections/all
• Category: SARMs, Supplements • Quality: Average •
Pricing: Overpriced • Verdict: Influencer bait. The products work,
but you're paying a massive premium to fund their marketing budget. Skip the
hype and buy from specialized labs.
IndiaMart http://www.indiamart.com
• Category: Industrial Bulk Raw Powders • Quality: High Risk
(Unregulated) • Pricing: Wholesale Floor • Verdict: This is a B2B
industrial site, not a retail shop. Buying small batches here is a gamble with
heavy metal contamination and underdosing. Unless you're an experienced chemist
with your own HPLC testing equipment, stay away.
─────────────────────────────────────────────────────
BODY
FAT
&
JAWLINE
DEFINITION
The Soft Tissue Drape • The Limits of Fat Loss • Neck Definition
First, let's determine the ideal body fat percentage for bone definition and clarity in the lower third. Before we go any further, we first need to understand what body fat actually is.
━━━━━━━━━━ ❖ WHAT IS BODY FAT? ❖ ━━━━━━━━━━
❖ WHAT IS BODY FAT? ❖ ━━━━━━━━━━
At its core, body fat is
triglycerides stored within adipocytes. Aesthetically, this subcutaneous adipose
tissue acts as a biological blur filter over your musculoskeletal
frame.
⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯
When your body fat percentage is high, this subcutaneous
layer thickens. It fills in natural facial depressions—like the submalar
space—and rounds out sharp skeletal landmarks. This masks muscle belly
separation and buries the defining contours of the skull, specifically the
zygomatic arch, the mandibular border, and the gonial angle.
⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯
As you lean out and those adipocytes shrink, this
overlying layer thins. The skin and superficial fascia drape tightly against the
underlying bone and muscle. That dramatic shift from a "soft" face to a
"chiseled" one isn't the result of your skeletal structure changing overnight.
It is the physical decompression of the tissue, letting the hard edges of your
skull dictate how light and shadow hit your
face.
I AM NOT WRITING A GUIDE TO LOSE BODY FAT THIS SHOULD BE SELF-EXPLANATORY. For P.E.D.S, to reduce BF%; Ages 13-18.
The Protocol:
Run this for 6-8 weeks max. You must be in a strict
caloric deficit.
Why did this section turn out like
such absolute garbage? Honestly, whatever. I'm over it, fuckass im not re-doing
this.
We’ve locked in the two highest-ROI structural shifts: lower-third development and skeletal definition.
Now, the focus turns to the high-yield softmaxes that tie the entire look together.
The Definitive Lower Third Softmaxxing
Compendium
A Complete Anatomical Guide to Non-Surgical Mandibular, Masseter, and
Mentalis Optimization
Note: Softmaxxing, will include Performance Enhancing drugs, although no surgery
Step 1: The Masticatory Load Protocol
(Masseter Hypertrophy & Condyle Remodeling)
Stop wasting money on cheap, soft chewing gum. It dissolves in minutes and simply does not provide the mechanical resistance required to trigger actual bone remodeling.
Material:
You need 100% natural mastic gum or high-resistance Falim gum. If you don't want to chew gum, force tough, heavily dehydrated foods into your diet—think biltong, thick cuts of tough meat, or raw carrots.
Routine:
Chew for 20 to 30 minutes every other day. Do not push past the 30-minute mark; overloading the joint just leads to TMJ inflammation, which will set your progress back.
Technique:
Only chew on your molars, and alternate sides with every bite to keep your facial development symmetrical. Keep your lips sealed shut. Crucially, do not use your cheeks (buccinator muscles) to move the gum around. Use your tongue. Relying on your cheeks will bloat your face, whereas tongue-driven chewing keeps the cheeks flat and hollow.
Step 2: Nighttime Airway Stabilization
(Mouth Taping)
Growth happens while you sleep. If you mouth-breathe at night, your jaw drops open, forcing a clockwise, downward growth pattern that ruins facial projection.
Material:
Get 3M Micropore medical tape. It does the job without ripping your skin off in the morning.
Routine:
Place a small vertical strip right over the center of your lips before bed. This physically forces nasal breathing throughout the night.
Prerequisite:
This only works if your nasal airway is actually clear. If you suffer from chronic allergies, hit your nose with a saline spray or throw on a nasal dilator strip first. Never tape your mouth shut if your nose is completely blocked.
Step 3: The Myofunctional Swallow
(Dynamic Tongue Posture)
Static "mewing" is practically useless if you still have an infantile swallow pattern. Infantile swallowing relies on the buccinator muscles to force food down. That pushes the dental arch inward while blowing out your cheeks, giving you a permanently bloated look.
Exercise:
The "Mona Lisa" Swallow.
Method:
Gather some saliva on top of your tongue. Pin the tip of your tongue against the alveolar ridge—that little bump just behind your front teeth—making sure you aren't actually touching the teeth themselves. Now press the entire body of your tongue, especially the posterior third, completely flat against the roof of your mouth. Swallow. Do it without moving your lips, your cheeks, or your neck muscles.
Frequency:
Force yourself to do this every single time you eat or drink. Eventually, this conscious mechanical effort rewires into your subconscious default swallow. When that happens, you start applying heavy forward and lateral force to your maxilla thousands of times a day.
Step 4: The Pharmacological Matrix
(Endocrine Puberty-Maxxing)
Chewing provides mechanical stress, which locally upregulates the Wnt/β-catenin pathway. However, systemic IGF-1 dictates the actual raw materials available for bone apposition. The strategy here is straightforward: spike your growth factors while simultaneously delaying growth plate fusion.
Compound A: MK-677 (Ibutamoren) - GH/IGF-1 Secretagogue
Mechanism:
MK-677 binds to the ghrelin receptor, commanding the pituitary gland to release massive pulses of endogenous HGH. This triggers a drastic elevation in systemic IGF-1, forcing your condylar cartilage into rapid proliferation right before endochondral ossification locks it in.
Theoretical Dose:
12.5mg orally, taken strictly before bed.
Tradeoffs & Coping:
Be warned: MK-677 drives up insulin resistance and causes heavy water retention. You will probably get "moon face" and look bloated during the cycle. That is the temporary tradeoff for permanent bone density. You have to monitor your fasting blood glucose. Cycle the compound (for example, 5 days on, 2 days off) so you don't permanently desensitize your pituitary gland.
Compound B: Exemestane (Aromasin) - Suicidal Aromatase Inhibitor
Mechanism:
Exemestane binds irreversibly to the aromatase enzyme. This shuts down the conversion of testosterone into estradiol (E2). Since high E2 is the exact signal that tells your body to calcify and fuse its growth plates, micro-dosing an AI artificially keeps that pubertal growth window open—buying you months, and sometimes years, of extra development.
Theoretical Dose:
6.25mg orally, taken every 3.5 days (twice a week).
Tradeoffs & Coping:
Do not completely nuke your E2. Flatlining your estrogen leads to severe joint desiccation (which means brutal TMJ pain when you chew), osteopenia, and heavy cognitive brain fog. The objective is to push E2 down into the low-normal reference range, not crash it to zero. Exemestane is the drug of choice over Arimidex because it prevents massive estrogen rebound the second you halt the cycle.
The Teen Jaw-Growth Protocol
Clinical Overview
At this age, your spheno-occipital synchondrosis and midfacial sutures haven't fully fused. This leaves a brief biological window for actual bone redirection—the primary factor dictating the length of your submental plane.
1. The Somatic Swallow Overlay
2. Hyoid Bone Anchoring
Past the age of 21, your craniofacial skeleton is fully fused. At this point, the bone isn't moving without a saw. Your entire focus must shift to shortening the resting length of the suprahyoid muscles and aggressively tightening the deep cervical fascia.
1. Mylohyoid Isometric Shortening
2. Digastric Muscle Atrophy via Agonist Overload
3. Deep Cervical Fascia Stretching
The Holy Grail of Softmaxxing
Optimizing the Lower Third: Soft Tissue Refinement & Facial Definition
Every inch of your jawbone is wrapped in the periosteum—a dense, highly reactive fibrous membrane. Subject the mandible to extreme mechanical stress, and
osteocytes buried deep within the bone matrix immediately detect the strain.
Yet, you inevitably hit a biological brick wall: Sclerostin.
Secreted directly by your osteocytes, this glycoprotein acts as an emergency brake on skeletal expansion. It completely paralyzes the Wnt/β-catenin signaling pathway, the precise molecular cascade responsible for laying down fresh bone.
Why? Because dense cortical bone requires immense metabolic energy, and your system is hardwired to fiercely resist building it.
Attempt to brute-force the issue by aggressively chewing hard food, and your body retaliates by dumping a flood of Sclerostin into the matrix.
The result?
You build massive, puffy masseter muscles that sit uselessly on top of the exact same narrow skeletal base. If you want true, bone-deep lateral flare, you must
biochemically crush local Sclerostin expression while simultaneously flooding the masseteric tuberosity with non-aromatizing androgens.
Phase I: Transverse Width (The Cortical Flare Matrix)
You cannot systemic-maxx your way to a wider jaw without destroying your organs
or mutating into a neanderthal. The strategy requires pinning the anabolic
signaling directly to the gonial angles.
Relying on DMSO as a carrier is biomechanical suicide. Because DMSO acts as a
universal penetrant, it instantly breaches the subdermal capillary networks and
flushes the DHT straight into systemic circulation—nuking your hairline and
swelling your prostate. To keep the androgen payload physically locked at the
periosteum, you need a liposomal encapsulation base.
Phase II: The Mechanical & Systemic Trigger
With the DHT locally pooled at the jawbone, you now have to force the actual
calcification.
1. The Sclerostin-Killer Stack: Administer 20mcg of Teriparatide (Forteo)
subcutaneously into the abdomen every morning. Alongside this, take 70mg of
Alendronate (a potent bisphosphonate) orally once a week. The Teriparatide
crushes local Sclerostin expression, giving the osteoblasts the green light
to construct new bone. Meanwhile, the Alendronate chemically paralyzes the
osteoclasts, ensuring that the newly formed matrix isn't instantly
reabsorbed. Cap this cycle at a strict 12-week maximum to mitigate any
osteosarcoma risks.
2. High-Density Isometrics (Stop Chewing): Endless dynamic chewing builds the
wrong muscle fibers (Type I), yielding a bulky, soft-looking masseter
profile. The objective is localized bone strain, not muscular hypertrophy.
Position a dense silicone block squarely between your rear molars. Bite down
at 90% of your absolute maximum force and hold that brutal static isometric
contraction for 45 seconds. Execute 5 sets per side, strictly every other day.
This extreme static load physically bends the mandible at a microscopic level,
generating the exact piezoelectric charge required to pull calcium directly into
the hydroxyapatite matrix.
Phase III: Sagittal Projection (Submental Fibrosis)
Once your skeletal structure fuses, your side profile is dictated by a single
variable: how tightly the soft tissue wraps beneath the mandible. If your hyoid
bone rests low, you are stuck with a permanent double chin.
Pumping the area full of fat-burners like Kybella simply destroys the adipose
tissue, leaving you with empty, loose skin draping off a recessed jaw. Instead,
the strategy is to intentionally induce localized scarring (fibrosis) to
physically shrink-wrap the submental fascia.
This is meant to produce a rip-off of a surgery such as trimax, although the results will defentiely be a lot diffrent.
also a risk of bone cancer, but liitle.
Link: https://looksmax.org/threads/hardmaxxing-lower-third.2228707/
"Can chewing mastic gum fix this?"
I asked, sliding a candid side-profile photo
across the desk. It highlighted my melting chin, the soft transition from jaw to
throat, and a complete absence of a gonial angle.
One of the top maxillofacial surgeons in the country just laughed, pulled up a
CBCT scan, and showed me exactly why my skull was the actual problem.
Since then, I’ve analyzed hundreds of scans, consulted with world-class
specialists, and helped dozens of guys on this board navigate surgery. I know
what actually works, and I'm tired of watching guys waste their prime on useless
orthotropics.
Here is the brutal truth: most "lower third" guides here are garbage. They are
written by fifteen-year-olds who think chewing hard gum or injecting some
peptides for two weeks will magically swing their mandible forward. It won’t,
JFL. If your skeletal structure is recessed, no amount of mewing is going to
save you once your growth plates are fully fused.
This thread is the definitive blueprint. I am laying out the exact mechanics of
the lower third by age group—because what works for a twelve-year-old with open
sutures will do absolutely nothing for a twenty-five-year-old with a locked
skull.
We are going to dissect:
- The biological reality of growth: Palate expansion (MSE/MARPE), functional
appliances, and the harsh mechanics of why traditional orthodontics probably
ruined your face in the first place.
- Soft tissue vs. bone: Why hitting a low body fat percentage won't save a
recessed jaw, and why jaw filler is just a puffy, temporary cope for a
compromised airway.
- The endocrinology of bone remodeling: How exogenous HGH and specific
androgenic-anabolic steroids (AAS) physically alter lower-third length and
expand bi-gonial width. I will separate the transient water retention of
masseter hypertrophy from actual skeletal thickening.
- Wolff's Law and bonesmashing: The clinical mechanics behind micro-fractures.
We’ll look at whether localized blunt-force trauma can realistically induce
forward projection, or if you are just begging for asymmetric calcification
and permanent facial disfigurement.
- Hardmaxxing: Sliding genioplasties, custom implants, and the specific
diagnostic markers that dictate when you actually need to drop the cash on a
full bimaxillary advancement (Bimax).
Stop wasting time on pseudo-science. Let's look at the actual anatomy.
appliances, and the harsh mechanics of why traditional orthodontics probably
ruined your face in the first place.
- Soft tissue vs. bone: Why hitting a low body fat percentage won't save a
recessed jaw, and why jaw filler is just a puffy, temporary cope for a
compromised airway.
- The endocrinology of bone remodeling: How exogenous HGH and specific
androgenic-anabolic steroids (AAS) physically alter lower-third length and
expand bi-gonial width. I will separate the transient water retention of
masseter hypertrophy from actual skeletal thickening.
- Wolff's Law and bonesmashing: The clinical mechanics behind micro-fractures.
We’ll look at whether localized blunt-force trauma can realistically induce
forward projection, or if you are just begging for asymmetric calcification
and permanent facial disfigurement.
- Hardmaxxing: Sliding genioplasties, custom implants, and the specific
diagnostic markers that dictate when you actually need to drop the cash on a
full bimaxillary advancement (Bimax).
Stop wasting time on pseudo-science. Let's look at the actual anatomy.
Section I: The Clinical Baseline — Why Your Mirror Is Lying to You
Stop staring in the bathroom mirror. If you're on this board, you've probably spent hours holding your phone at head-height, tilting your chin up at a 45-degree angle under downlight, trying to convince yourself that your lack of a jawline is just water retention. It’s a massive cope. Mirror frauding doesn't change your skeletal reality.
"My jaw looks decent when I jut my mandible forward, but my side profile looks melted in candid photos. Do I just need to lose face fat?"
JFL. If you have to thrust your jaw forward to look normal, you have a structural deficit. Let's look at the actual physics of why you look like a thumb in unposed photos.
Front-facing phone cameras use wide-angle lenses, usually a 26mm to 28mm equivalent. At close range, this focal length warps 3D geometry—it stretches the center of your face forward (making your nose look huge) while shrinking the sides, narrowing your perceived bi-gonial width.
Conversely, a candid shot from 10 feet away on a telephoto lens (an 85mm to 105mm equivalent) compresses facial depth and shows your actual skeletal projection.
If you want a real diagnosis, put the phone down. Your only real entry points are a lateral cephalogram or a 3D CBCT scan. These completely eliminate optical distortion so you can map out your actual skull landmarks.
Conversely, a candid shot from 10 feet away on a telephoto lens (an 85mm to 105mm equivalent) compresses facial depth and shows your actual skeletal projection.
If you want a real diagnosis, put the phone down. Your only real entry points are a lateral cephalogram or a 3D CBCT scan. These completely eliminate optical distortion so you can map out your actual skull landmarks.
Bone vs. Soft Tissue: The Scaffold and the Drape
Before measuring angles, you must understand the relationship between the bone scaffold and the soft tissue drape. Most guys on this board fail to make this distinction.The maxilla is your facial foundation, locked directly into the skull. The mandible is a separate bone suspended by muscles, ligaments, and joints. Your chin is merely a small projection on the front of that mandible—it is not the jaw itself.
Draped over this bone scaffold is your soft tissue: skin, fat pads, the platysma muscle, masseters, and submental tissue. While soft tissue can temporarily camouflage mild skeletal recessions, soft tissue cannot fundamentally change where your bones sit. If your underlying bone framework lacks projection, your soft tissues will sag, bunch up, and melt into your neck. You cannot solve a structural volume deficit with fat-loss or topical tricks.
SNA/SNB Angles & The Downward Swing
If your face is long, narrow, and flat, your skull grew vertically instead of horizontally. Maxillofacial surgeons measure this using specific angles on a lateral cephalogram.| Landmark / Angle | Aesthetic Norm | Clinical Relevance |
| SNA Angle | 82° ± 2° | Maxillary projection. Low numbers mean a recessed midface. |
| SNB Angle | 80° ± 2° | Mandibular projection. Dictates chin recession. |
| ANB Angle | 2° | The gap between jaws. High numbers indicate severe retrognathia. |
| FMA (Frankfort-Mandibular Plane Angle) | 25° or lower | Vertical jaw tilt. High FMA means a steep, downward-swung profile. |
If your FMA is 35° or higher, your gonial angle is virtually non-existent. You can chew mastic gum until your masseters look like golf balls, but because the bone is tilted down, those muscles will just bulge outward and sag, giving you a bloated, puffy lower face rather than a sharp jawline. Do not chew hard gum if you have a high FMA—it will only increase your facial height."A high mandibular plane angle (FMA > 30°) is consistently correlated with a lack of chin projection, an obtuse gonial angle, and an apparent shortening of the ramus height." (Proffit et al., Contemporary Orthodontics)
The Airway and the Hyoid Penalty
Ever wonder why skinny, recessed guys still have a soft, double-chin profile? It's a survival mechanism.When your mandible is recessed (an SNB below 76°), your tongue and soft palate get shoved back toward your spine, choking your airway. On a lateral ceph, a healthy airway is 10mm to 12mm wide. If yours is choked down to 6mm, you're borderline suffocating.
To keep you breathing, your brain drops your hyoid bone—the free-floating bone anchoring your tongue—down and back to open up the airway.
This drop drags the surrounding soft tissue down with it, creating that sloping, melted neck-to-chin line. You can starve yourself down to 8% body fat, but you'll never get a sharp 90-degree submental angle. The skin can't tighten because the bone scaffold is too far back. Never try to starve away a double chin caused by a recessed mandible; you'll just look emaciated with the exact same soft neck.
If you had braces as a teen, your orthodontist might have wrecked your facial development to "fix" an overbite. This is camouflage orthodontics. Instead of advancing your weak lower jaw, they dragged your upper teeth backward to meet it.
Check your dental history for these red flags:
Check your dental history for these red flags:
- Four premolar extractions (two upper, two lower) to fix crowding.
- Retraction headgear or heavy Class II elastics to pull your front teeth back.
- A narrow, V-shaped upper dental arch instead of a wide, U-shaped one.
- A flat, sunken-in upper lip and early nasolabial creases.
If your scans show a steep FMA and a choked airway, your lower third is a skeletal issue. Stop wasting money on face rollers and soft-maxxing copes. The bone has to move. Let's look at how we actually change the skeletal frame.
What is the lower third?
The lower third is the anatomical region spanning from the base of the nose (subnasale) to the lowest
point of the chin (menton), defining both your vertical facial proportions and
horizontal skeletal projection. Frontally, it dictates your bi-gonial width and
lower jaw symmetry, while your profile relies entirely on the mandible's forward
projection, gonial angle, and submental sharpness. Beyond pure aesthetics, this
bone scaffold supports your airway and soft-tissue drape, making a highly
projected lower third the single most dominant marker of masculine facial
strength.
The lower third is the anatomical region spanning from the base of the nose (subnasale) to the lowest
point of the chin (menton), defining both your vertical facial proportions and
horizontal skeletal projection. Frontally, it dictates your bi-gonial width and
lower jaw symmetry, while your profile relies entirely on the mandible's forward
projection, gonial angle, and submental sharpness. Beyond pure aesthetics, this
bone scaffold supports your airway and soft-tissue drape, making a highly
projected lower third the single most dominant marker of masculine facial
strength.
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
SECTION II: THE SKELETAL TIMELINE
Palatal Expansion, Mid-Palatal Sutures, and the Orthodontic Trap
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
THE SKULL IS LOCKED. YOU CANNOT FORCE IT.
SECTION II: THE SKELETAL TIMELINE
Palatal Expansion, Mid-Palatal Sutures, and the Orthodontic Trap
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
THE SKULL IS LOCKED. YOU CANNOT FORCE IT.
Trying to widen or advance a fused skull with your tongue or hard gum is a losing battle against basic physics. Your skull is not a soft lump of clay. It is a highly secure system of solid bones locked together by fibrous joints called sutures [2]. As you age, these sutures undergo interdigitation—they twist, mesh, and eventually fuse into solid, unmovable bone (synostosis).
THE "GROWTH PLATE" MYTH
Before looking at appliances, let's clear up some basic anatomy. Half the guys on this forum throw around the term "growth plates" when talking about the jaw. JFL.
Your mandible is not a femur. Long bones grow in length via endochondral ossification at epiphyseal growth plates. Your jaws do not have these.
Long bones grow in length via endochondral ossification at epiphyseal growth plates. Your jaws do not have these.
• The Upper Jaw (Maxilla):
Grows entirely via intramembranous ossification. Bone is deposited directly into the fibrous tissue of your facial sutures and onto the outer surfaces of the bone [1.2.7].
• The Lower Jaw (Mandible):
It grows primarily through surface remodeling, but has a unique growth site at the head of the jaw joint: the condylar cartilage [1.1.2, 1.2.6]. This is secondary cartilage [1.1.2]. It does not have an independent, genetically predetermined growth clock like a primary growth plate [1.1.2]. Instead, it is highly reactive to mechanical load, posture, and local environment during your development years [1.1.2].
Code:
LONG BONE GROWTH MANDIBULAR GROWTH
(Epiphyseal Plates) (Sutures & Condylar Drift)
[Epiphysis] \ Condyle / <-- Secondary Cartilage
============= \ /
[Growth Plate] | Ramus | <-- Deposition (Back)
------------- | | <-- Resorption (Front)
[Diaphysis] / Body \
[ Chin ] <-- Appositional Growth• The Upper Jaw (Maxilla):
Grows entirely via intramembranous ossification. Bone is deposited directly into the fibrous tissue of your facial sutures and onto the outer surfaces of the bone [1.2.7].
• The Lower Jaw (Mandible):
It grows primarily through surface remodeling, but has a unique growth site at the head of the jaw joint: the condylar cartilage [1.1.2, 1.2.6]. This is secondary cartilage [1.1.2]. It does not have an independent, genetically predetermined growth clock like a primary growth plate [1.1.2]. Instead, it is highly reactive to mechanical load, posture, and local environment during your development years [1.1.2].
CLINICAL REALITY
Your jaw growth plates didn't "close" because they never existed.
What actually happened:
• Sutures fused [1.1.2]
• Condylar cartilage lost its adaptive capacity [1.1.2]
• Cortical bone hardened into concrete
This means your biological age dictates your exact treatment matrix.
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
The Age-Bracket Matrix: What Actually Works
What options are biologically viable for you right now?
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Bracket 1: The Pediatric Window (Age 14 and Under)
Sutures Open — Angelieri Stage A or B
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
• The Strategy: Functional appliances (like the Twin Block or Herbst appliance) can encourage the mandible to grow forward by holding it in a protruded position, stimulating the highly reactive condylar cartilage. Reverse-pull face masks can pull a recessed maxilla forward.
• The Reality: If you are in this age bracket, you have a massive advantage. You do not need surgery; you need an airway-focused orthodontist who understands horizontal growth.
Bracket 2: The Transitional Phase (Age 15 to 20)
Interdigitated Sutures — Angelieri Stage C
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
• The Strategy: Standard orthodontics will no longer work; they will simply tip your teeth outward . To expand the upper jaw, you need high-force skeletal expansion, specifically MARPE (Miniscrew-Assisted Rapid Palatal Expansion) or MSE (Maxillary Skeletal Expander).
• The Reality: The expander is anchored directly to the palatal bone using four titanium miniscrews (TADs). When you turn the expansion screw, the force bypasses the teeth and goes straight to the bone, splitting the mid-palatal suture down the middle. If successful, a gap (diastema) will open between your front teeth, proving true skeletal expansion.
Bracket 3: The Skeletal Lock (Age 21+)
Sutures Fully Fused — Angelieri Stage D and E

━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
• The Strategy: Forcing an MSE at this age without surgical assistance has a high failure rate. You risk tilting the anchor pins, bending the expander, or causing severe localized bone loss. To expand the upper jaw, you need surgically assisted rapid palatal expansion (SARPE) or a surgical split like DOME (Distraction Osteogenesis Maxillary Expansion) . For the lower jaw, you cannot "expand" the bone itself without distraction osteogenesis (MDO) because the mandible is a single, solid bone with no midline suture to split.
• The Reality: You are in hardmaxxing territory. Your choices are either bone-borne expansion devices with surgical corticotomies (micro-fracturing the bone to allow movement) or full jaw surgery.
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
The Mewing Math: Tongue Pressure vs. Cortical Resistance
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
The internet has convinced guys that "mewing" (keeping the tongue on the roof of the mouth) can swing the entire maxilla upward and forward. Let's look at the actual physics:
• Tongue Force Output: The human tongue can exert a light, continuous lateral force of roughly 0.1 to 0.2 Newtons. This is only enough to slowly shift teeth (dental tipping) over months because teeth sit in a dynamic periodontal ligament.
• Sutural Separation Threshold: Splitting a mature midpalatal suture requires a force threshold of 80 to 120 Newtons.
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
The Age-Bracket Matrix: What Actually Works
What options are biologically viable for you right now?
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Bracket 1: The Pediatric Window (Age 14 and Under)
Sutures Open — Angelieri Stage A or B
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
• The Strategy: Functional appliances (like the Twin Block or Herbst appliance) can encourage the mandible to grow forward by holding it in a protruded position, stimulating the highly reactive condylar cartilage. Reverse-pull face masks can pull a recessed maxilla forward.
• The Reality: If you are in this age bracket, you have a massive advantage. You do not need surgery; you need an airway-focused orthodontist who understands horizontal growth.
Bracket 2: The Transitional Phase (Age 15 to 20)
Interdigitated Sutures — Angelieri Stage C
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
• The Strategy: Standard orthodontics will no longer work; they will simply tip your teeth outward . To expand the upper jaw, you need high-force skeletal expansion, specifically MARPE (Miniscrew-Assisted Rapid Palatal Expansion) or MSE (Maxillary Skeletal Expander).
• The Reality: The expander is anchored directly to the palatal bone using four titanium miniscrews (TADs). When you turn the expansion screw, the force bypasses the teeth and goes straight to the bone, splitting the mid-palatal suture down the middle. If successful, a gap (diastema) will open between your front teeth, proving true skeletal expansion.
Bracket 3: The Skeletal Lock (Age 21+)
Sutures Fully Fused — Angelieri Stage D and E
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
• The Strategy: Forcing an MSE at this age without surgical assistance has a high failure rate. You risk tilting the anchor pins, bending the expander, or causing severe localized bone loss. To expand the upper jaw, you need surgically assisted rapid palatal expansion (SARPE) or a surgical split like DOME (Distraction Osteogenesis Maxillary Expansion) . For the lower jaw, you cannot "expand" the bone itself without distraction osteogenesis (MDO) because the mandible is a single, solid bone with no midline suture to split.
• The Reality: You are in hardmaxxing territory. Your choices are either bone-borne expansion devices with surgical corticotomies (micro-fracturing the bone to allow movement) or full jaw surgery.
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
The Mewing Math: Tongue Pressure vs. Cortical Resistance
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
The internet has convinced guys that "mewing" (keeping the tongue on the roof of the mouth) can swing the entire maxilla upward and forward. Let's look at the actual physics:
• Tongue Force Output: The human tongue can exert a light, continuous lateral force of roughly 0.1 to 0.2 Newtons. This is only enough to slowly shift teeth (dental tipping) over months because teeth sit in a dynamic periodontal ligament.
• Sutural Separation Threshold: Splitting a mature midpalatal suture requires a force threshold of 80 to 120 Newtons.
CLINICAL IMPLICATION
Your tongue is literally three orders of magnitude too weak to overcome the resistance of your facial sutures.
When you mew as an adult, you are merely pushing your upper teeth outward, which leads to alveolar bone loss, gum recession, and flared incisors. It is a biological impossibility to split a fused suture with soft tissue.
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Skeletal Expansion vs. Dental Tipping
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━[/CENTER>
Most orthodontists are lazy. When an adult patient has a narrow palate and a crossbite, the orthodontist will often use a standard quad-helix or a rapid palatal expander (RPE) anchored solely to the teeth.
In a grown adult, this does not expand the jawbone. It causes dental tipping.
The Dental Tipping Trap: Why Orthodontists Ruin Faces
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Code:
SKELETAL EXPANSION DENTAL TIPPING
(True Width) (Weak / Receded)
| | | \ | /
===[SUTURE]=== ====[SUTURE]====
| | | / | \
[Bone Splits] [Teeth Flare Out]When teeth are tipped outward to make the dental arch look wider, the roots of the teeth are forced against the thin outer plate of the jawbone (the buccal cortex).
This causes severe structural damage:
• Gingival recession: The gums shrink away from the tilted teeth.
• Bone loss (Dehiscence): The tooth root physically pushes through the bone envelope.
• Unstable occlusion: The moment you take your retainer out, your teeth instantly collapse back inward.
THE BOTTOM LINE
If you are planning to widen your palate to gain cheekbone support, widen your nasal cavity, and create room for your tongue, you must demand a bone-anchored device (MSE/MARPE).
If your orthodontist tells you that a plastic clear aligner or a basic wire retainer can expand your skeletal palate as an adult, leave their office immediately. They are treating your skeleton like a set of crooked teeth.
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
SECTION III: THE HORMONAL ARCHITECTURE
Androgens, Bone Remodeling, and the Limits of Endocrine Enhancement
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
"Can topical DHT grow my chin?" "Will MK-677 swing my mandible forward?"
SECTION III: THE HORMONAL ARCHITECTURE
Androgens, Bone Remodeling, and the Limits of Endocrine Enhancement
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
"Can topical DHT grow my chin?" "Will MK-677 swing my mandible forward?"
Every single day, my inbox gets trashed with blurry, down-lit side profiles from guys looking for a cheap shortcut. Drunk on TikTok "hormone-maxxing" trends, they genuinely believe a vial of liquid Masteron or a handful of research peptides is going to chemically rescue a recessed lower third and turn them into Chico.
It won't.
Let's look at the actual clinical endocrinology. Your skeleton isn't static rock. It is highly active metabolic tissue. But your ability to remodel that bone is entirely dictated by the biological clock of your secondary cartilages and the site-specific density of your androgen receptors (AR).
The Receptor Map: Why the Jaw is Unique
The craniofacial complex doesn't react to sex steroids the same way the rest of your body does. A femur or clavicle has a standard baseline of androgen receptors. The mandibular condyle, masseter attachment sites, and the cortical plates of the mandible? They are dense, hyper-reactive hotbeds for AR expression.
In vitro assays of human osteoblastic cells (HOCs) prove this. Cells pulled from the mandible express up to three times the AR mRNA of those taken from the axial skeleton.
Kasperk said:"We examined AR mRNA expression, androgen binding sites, and mitogenic responses to the androgen dihydrotestosterone (DHT) in human osteoblastic cell (HOC) populations... Mandibular and cortical HOC of both sexes expressed higher AR mRNA levels, significantly more androgen binding sites per cell, and exhibited significantly greater mitogenic responses to DHT than iliac crest-derived and trabecular HOC of the same skeletal system."
— Skeletal site-dependent expression of the androgen receptor in human osteoblastic cell populations. Calcified Tissue International, 61(5), 369-373.
This intense, localized receptor density is what actually drives the sexual dimorphism of the male skull. It creates the flared gonial angle, the lateral ramus width, the forward projection of the chin, and the heavy brow ridge. Dihydrotestosterone (DHT) carves out these traits, but it only does so during highly specific developmental windows.
Once your skeletal sutures and cartilaginous zones fuse, the door slams shut.
The Lower Third Blueprint: Length vs. Width
Before you even think about pinning anything, you need to define what "growing your jaw" means for your specific skull. Fixing a recessed lower third requires manipulating two entirely different vectors of bone growth. Each is governed by different chemical stacks and biological limits.
- Vector 1: Sagittal & Vertical Length (Fixing a Short Lower Third). If your face looks mathematically compressed from the bottom of your nose to your chin, your lower facial third is deficient. You have to physically lengthen the mandible so it drops downward and swings forward. This is ONLY possible during the 16–18 age window. The pubertal stack detailed below aims specifically at the condylar cartilage, generating true longitudinal growth to permanently extend the bone.
- Vector 2: Transverse Width (Creating Jaw Flare). If your lower third is an ideal length but lacks angularity from the front, you need lateral mass. You can do this at any age (21+). The adult cortical flare stack doesn't lengthen the bone. Instead, it uses mechanical stress and DHT derivatives to pack dense appositional bone onto the outer plates of the gonial angles.
The Temporal Windows: Puberty vs. Fused Adulthood
Stop guessing based on your chronological age. Look at the biological markers.
| Developmental Phase | Biological Marker | Maximum Skeletal Potential | Primary Chemical Drivers |
|---|---|---|---|
| Late Puberty (Ages 16–18) | Interdigitated sutures; active condylar cartilage | Longitudinal lengthening of mandible; ramus height increase | Growth Hormone (GH), IGF-1, DHT |
| Early Adulthood (Ages 19–21) | Fully interdigitated sutures; mineralizing condyle | Minimal longitudinal lengthening; high appositional thickening | DHT, Growth Hormone (low dose) |
| Fused Adult (Ages 22+) | Complete synostosis; mineralized condylar cartilage | Zero longitudinal growth. Pure appositional cortical thickening | DHT (appositional), mechanical loading |
The Late Pubertal Salvage Window (Ages 16–18)
If you're in this bracket, your long bone epiphyseal plates are basically done. But you have a biological loophole: the secondary cartilage of the mandibular condyle is still metabolically active. This specific cartilage bypasses standard endochondral ossification and responds aggressively to mechanical strain and systemic GH/IGF-1 levels.
Deploying highly androgenic, non-aromatizing compounds alongside recombinant growth hormone (rhGH) during this narrow window forces the condyle to lay down new bone.
The absolute dealbreaker? Estrogen. Estrogen (E2) drives growth plate fusion and condylar mineralization in both sexes. If you run heavily aromatizing cycles—like high-dose testosterone—you will spike your systemic E2, instantly fuse your growth zones, and permanently lock your mandible into its recessed state.
Core Objective: Total exploitation of the secondary
fibrocartilage of the mandibular condyle via systemic IGF-1 saturation, targeted
AR-upregulation, and aggressive Piezo1-mediated mechanotransduction. We are
forcing endochondral ossification in a race against epiphyseal closure. Failure
to maintain the precise E2 window results in premature fusion (bone-lock) and
permanent sub-tier mandibular deficiency.
The Endocrine & Growth Axis (The Engine)
Human Chorionic Gonadotropin (hCG): 250 IU SubQ Every Other Day (EOD).
Mechanical Spec: 31G 5/16" needle, shallow subcutaneous. Clinical Logic:
Absolute requirement to maintain intratesticular testosterone. Without this, the
Anavar-induced LH suppression crashes E2, triggering immediate chondrocyte
apoptosis. Zero E2 = zero growth.
rhGH (Somatropin): 5.0 IU Daily. Administration: Split into 2.5 IU (06:00
Fasted) and 2.5 IU (22:00). Pharmacokinetics: Twice-daily dosing minimizes the
renal clearance spike associated with high-dose single boluses and maintains a
steady-state hepatic IGF-1 transcription rate. This avoids the receptor
downregulation seen in v4.0's IM protocol.
Exemestane (Aromasin): 6.25 mg Every Other Day (EOD). Titration: Strictly
modulated via LC/MS-MS bloodwork to maintain serum Estradiol (E2) between 20–30
pg/mL. Failure Mode: If E2 drops below 15 pg/mL, collagenase is upregulated and
the condylar cartilage becomes brittle, leading to irreversible fusion. If E2
exceeds 40 pg/mL, you risk premature epiphyseal closure. Precision is the only
option.
Oxandrolone (Anavar): 40 mg Daily. Dosing: Split into 13.3 mg doses every 8
hours (TID). Mechanism: Leverages the \approx 9.4\text{h} terminal half-life to
maintain saturation of androgen receptors (AR) in osteoblast-like cells. This
drives the proliferation of the hypertrophic zone within the condylar cartilage,
accelerating the conversion of cartilage to bone.
T4/T3 Blend (Levothyroxine/Liothyronine): 50 mcg T4 / 12.5 mcg T3 Daily (AM).
Logic: Mandibular condyles rely on localized Type II deiodinase (D2) for the
conversion of T4 \rightarrow T3. Without systemic T4, the avascular zones of the
condyle lack the substrate for TR\alpha1 receptor activation, stalling the final
stage of chondrocyte hypertrophy.
The Mechanotransduction Vector (The Direction)
Hormones provide the raw material; mechanical strain provides the blueprint.
Bite-Jumping Appliance (Herbst/MARA): Fixed mandibular advancement. Mechanism:
Creates continuous tensile strain on the retrodiscal tissues. This opens Piezo1
mechanosensitive ion channels, triggering the \text{Wnt}/\beta\text{-catenin}
pathway, which instructs the IGF-1 saturated chondrocytes to expand linearly.
LIPUS (Low-Intensity Pulsed Ultrasound): 1.5 MHz at 30 mW/cm². Application: 20
minutes daily, direct contact over the TMJ capsule. Clinical Effect: Acoustic
cavitation increases localized \text{COX-2} and \text{PGE2} expression,
exponentially increasing the sensitivity of the cartilage matrix to the tensile
forces of the Herbst appliance.
Masticatory Loading: High-resistance mastication (Hard Mastic Gum). Execution:
Strictly performed post-LIPUS. Logic: Compressive piezoelectric signaling is
required to densify the newly formed osteoid matrix. Without this, the growth is
structurally weak and prone to postoperative relapse.
The Bone Matrix Substrates (The Bricks)
- Strontium Ranelate: 680 mg daily. Take at 22:00, 4 hours post-calcium.
Ranelate is superior to Citrate for inhibiting osteoclast resorption while
simultaneously stimulating osteoblasts via the CaSR receptor.
- Vitamin K2 (MK-4): 5,000 mcg daily. Essential for the
\gamma\text{-carboxylation} of osteocalcin. MK-7 is insufficient for this
specific high-turnover skeletal protocol.
- Vitamin D3: 10,000 IU daily. Taken with dietary lipids to ensure intestinal
absorption.
- Choline-Stabilized Orthosilicic Acid (ch-OSA): 10 mg daily. Directly
increases the cross-linking density of Type-1 collagen in the
fibrocartilaginous mesh.
- Glucosamine Sulfate: 1,500 mg daily. Provides the requisite precursors for
glycosaminoglycan (GAG) synthesis.
- Collagen Type II (Undenatured): 40 mg daily. Specifically targets the
condylar fibrocartilage to prevent matrix degradation during aggressive
expansion.
Aesthetic Failure Modes
1. The E2 Crash: Skipping hCG or overdosing Exemestane leads to "bone-lock."
The plates fuse, and your lower third is permanently stunted.
2. The Soft-Tissue Trap: Running rhGH without the Herbst/LIPUS vector results
in acromegalic soft-tissue thickening (thick lips, widened nose) without any
actual skeletal lengthening.
3. The Metabolic Crash: Using T3 monotherapy without T4 leads to systemic
catabolism and localized cartilage atrophy.
Execute with clinical sterility. Any deviation from the E2 window is a permanent
aesthetic botch.
fibrocartilage of the mandibular condyle via systemic IGF-1 saturation, targeted
AR-upregulation, and aggressive Piezo1-mediated mechanotransduction. We are
forcing endochondral ossification in a race against epiphyseal closure. Failure
to maintain the precise E2 window results in premature fusion (bone-lock) and
permanent sub-tier mandibular deficiency.
The Endocrine & Growth Axis (The Engine)
Human Chorionic Gonadotropin (hCG): 250 IU SubQ Every Other Day (EOD).
Mechanical Spec: 31G 5/16" needle, shallow subcutaneous. Clinical Logic:
Absolute requirement to maintain intratesticular testosterone. Without this, the
Anavar-induced LH suppression crashes E2, triggering immediate chondrocyte
apoptosis. Zero E2 = zero growth.
rhGH (Somatropin): 5.0 IU Daily. Administration: Split into 2.5 IU (06:00
Fasted) and 2.5 IU (22:00). Pharmacokinetics: Twice-daily dosing minimizes the
renal clearance spike associated with high-dose single boluses and maintains a
steady-state hepatic IGF-1 transcription rate. This avoids the receptor
downregulation seen in v4.0's IM protocol.
Exemestane (Aromasin): 6.25 mg Every Other Day (EOD). Titration: Strictly
modulated via LC/MS-MS bloodwork to maintain serum Estradiol (E2) between 20–30
pg/mL. Failure Mode: If E2 drops below 15 pg/mL, collagenase is upregulated and
the condylar cartilage becomes brittle, leading to irreversible fusion. If E2
exceeds 40 pg/mL, you risk premature epiphyseal closure. Precision is the only
option.
Oxandrolone (Anavar): 40 mg Daily. Dosing: Split into 13.3 mg doses every 8
hours (TID). Mechanism: Leverages the \approx 9.4\text{h} terminal half-life to
maintain saturation of androgen receptors (AR) in osteoblast-like cells. This
drives the proliferation of the hypertrophic zone within the condylar cartilage,
accelerating the conversion of cartilage to bone.
T4/T3 Blend (Levothyroxine/Liothyronine): 50 mcg T4 / 12.5 mcg T3 Daily (AM).
Logic: Mandibular condyles rely on localized Type II deiodinase (D2) for the
conversion of T4 \rightarrow T3. Without systemic T4, the avascular zones of the
condyle lack the substrate for TR\alpha1 receptor activation, stalling the final
stage of chondrocyte hypertrophy.
The Mechanotransduction Vector (The Direction)
Hormones provide the raw material; mechanical strain provides the blueprint.
Bite-Jumping Appliance (Herbst/MARA): Fixed mandibular advancement. Mechanism:
Creates continuous tensile strain on the retrodiscal tissues. This opens Piezo1
mechanosensitive ion channels, triggering the \text{Wnt}/\beta\text{-catenin}
pathway, which instructs the IGF-1 saturated chondrocytes to expand linearly.
LIPUS (Low-Intensity Pulsed Ultrasound): 1.5 MHz at 30 mW/cm². Application: 20
minutes daily, direct contact over the TMJ capsule. Clinical Effect: Acoustic
cavitation increases localized \text{COX-2} and \text{PGE2} expression,
exponentially increasing the sensitivity of the cartilage matrix to the tensile
forces of the Herbst appliance.
Masticatory Loading: High-resistance mastication (Hard Mastic Gum). Execution:
Strictly performed post-LIPUS. Logic: Compressive piezoelectric signaling is
required to densify the newly formed osteoid matrix. Without this, the growth is
structurally weak and prone to postoperative relapse.
The Bone Matrix Substrates (The Bricks)
- Strontium Ranelate: 680 mg daily. Take at 22:00, 4 hours post-calcium.
Ranelate is superior to Citrate for inhibiting osteoclast resorption while
simultaneously stimulating osteoblasts via the CaSR receptor.
- Vitamin K2 (MK-4): 5,000 mcg daily. Essential for the
\gamma\text{-carboxylation} of osteocalcin. MK-7 is insufficient for this
specific high-turnover skeletal protocol.
- Vitamin D3: 10,000 IU daily. Taken with dietary lipids to ensure intestinal
absorption.
- Choline-Stabilized Orthosilicic Acid (ch-OSA): 10 mg daily. Directly
increases the cross-linking density of Type-1 collagen in the
fibrocartilaginous mesh.
- Glucosamine Sulfate: 1,500 mg daily. Provides the requisite precursors for
glycosaminoglycan (GAG) synthesis.
- Collagen Type II (Undenatured): 40 mg daily. Specifically targets the
condylar fibrocartilage to prevent matrix degradation during aggressive
expansion.
Aesthetic Failure Modes
1. The E2 Crash: Skipping hCG or overdosing Exemestane leads to "bone-lock."
The plates fuse, and your lower third is permanently stunted.
2. The Soft-Tissue Trap: Running rhGH without the Herbst/LIPUS vector results
in acromegalic soft-tissue thickening (thick lips, widened nose) without any
actual skeletal lengthening.
3. The Metabolic Crash: Using T3 monotherapy without T4 leads to systemic
catabolism and localized cartilage atrophy.
Execute with clinical sterility. Any deviation from the E2 window is a permanent
aesthetic botch.
The Adult Reality: Appositional Growth (Age 21+)
Once you hit 21, the game completely changes. Condylar cartilage? Mineralized. Sutures? Locked. You cannot chemically lengthen your lower third past this point. Period.
Blasting high-dose GH or IGF-1 as an adult won't buy you a single millimeter of forward mandibular length. You're just asking for localized acromegaly. Because the bone can no longer grow longitudinally, the excess GH forces appositional growth. Your skeleton just gets thicker. You walk away with heavy orbital rims, a bloated brow ridge, and massive hands.
The soft-tissue changes are even worse. GH abuse causes macroglossia (tongue expansion). The muscle pushes against your teeth, blowing out massive gaps (diastemas) and forcing your mouth into a flared, "chimp-lip" profile. Your nasal cartilage coarsens. Your skin gets thick and oily. You completely wreck your facial aesthetics.
But adult androgen-driven appositional growth is still highly viable for engineering lateral jaw flare. By targeting the cortical bone of the gonial angles, you can physically widen your lower third.
This protocol uses mechanotransduction. You combine extreme local mechanical strain (chewing) with non-aromatizing androgens to force localized osteoblastic activity at the masseteric tuberosity.
Underlying Mechanism: Heavy, high-resistance chewing induces localized micro-strain across the cortical bone of the gonial angle. This physical stress triggers osteoblast recruitment. Add potent androgenic signaling to the mix, and those osteoblasts start packing on new layers of bone.
The Stack:
Aesthetic Failure Modes: Do you have a steep Frankfort-Mandibular Plane Angle (FMA over 30°)? If so, this protocol will ruin your face. Masseteric hypertrophy will flare outward, but on a downward-swung jaw, you end up with a wide, bloated, bottom-heavy "pear" shape instead of a sharp mandible.
Underlying Mechanism: Heavy, high-resistance chewing induces localized micro-strain across the cortical bone of the gonial angle. This physical stress triggers osteoblast recruitment. Add potent androgenic signaling to the mix, and those osteoblasts start packing on new layers of bone.
The Stack:
- Drostanolone Propionate (Masteron): 150 mg per week, pinned as daily intramuscular micro-injections (approx. 21 mg/day) using a 29G 1/2" insulin syringe in the delt or vastus lateralis. Daily pinning keeps serum levels flat, preventing receptor downregulation.
- Primobolan Enanthate (Methenolone Enanthate): 150 mg to 200 mg per week. Primo is a highly tissue-selective, non-aromatizing base that works synergistically with Masteron to crank up collagen synthesis and bone mineral deposition in the cortical plates.
- Mechanical Loading (Chewing with Progressive Overload): 30 minutes of targeted, high-resistance chewing (food-grade silicone blocks or hard mastic gum) every other day. Treat it exactly like weightlifting. Warm up, hit high-tension holds, and push for progressive overload. Never chew daily. Bone remodeling demands a recovery phase.
- The Bone-Mineralization Matrix:
- Vitamin D3: 10,000 IU daily.
- Vitamin K2 (as MK-4): 5 mg to 15 mg daily. MK-4 is non-negotiable. It activates osteocalcin, the protein that binds calcium directly to the bone matrix. This ensures the calcium deposits into your stressed jawbone, not your arterial walls.
- Calcium (Elemental): 1,000 mg daily.
- Biological Hard-Stops:
- Drop the protocol immediately if your hematocrit climbs above 52%.
- Run monthly lipid panels. Drostanolone and Primobolan will trash your HDL. If it drops below 30 mg/dL, abort.
Aesthetic Failure Modes: Do you have a steep Frankfort-Mandibular Plane Angle (FMA over 30°)? If so, this protocol will ruin your face. Masseteric hypertrophy will flare outward, but on a downward-swung jaw, you end up with a wide, bloated, bottom-heavy "pear" shape instead of a sharp mandible.
Topical DHT & Peptides: The Greycel Cope
Let's bury the main DIY forum cope right now: smearing DHT cream (like Andractim) directly on your jawline.
It shows a massive misunderstanding of how transdermal pharmacokinetics and skeletal biology actually work.
- The Systemic Dilution: Transdermal DHT doesn't magically sit on the bone underneath the skin. It absorbs through the stratum corneum, hits the subdermal capillary beds, and washes straight into systemic circulation. You achieve the exact same skeletal receptor binding whether you rub the cream on your jaw, your shoulder, or the bottom of your foot.
- The Dalton's 500 Rule: DHT's molecular weight is 290.4 g/mol, so it crosses the skin barrier easily. But the actual dosages required to trigger adult bone remodeling far exceed local receptor saturation limits. Instead of a wider jaw, you just get patchy beard growth, accelerated baldness, and a shut-down endocrine axis.
- Peptide Pulsing vs. Steady-State: Trying to grow bone with GHRHs or GHRPs like CJC-1295 or Ipamorelin is pointless. These compounds just create brief, transient pulses of growth hormone. Great for deep sleep and mild fat loss, useless for skeletal architecture. Real bone remodeling demands sustained, elevated serum levels of IGF-1 over months.
The Non-Surgical Alternative: Beard Frauding
If your bones are fused, you missed the pubertal window, and a $20k BSSO/genioplasty is out of the question, you have exactly one non-surgical option left to fix a compressed lower third: Beard Frauding.
By cultivating dense facial hair (using 5% topical Minoxidil and a 1.5mm dermaroller if your genetics are trash), you can visually reconstruct your facial thirds. Keep the cheek lines trimmed tight to preserve zygomatic definition, but let the hair on the chin and jawline grow out. By edging the bottom line a centimeter below your actual mandible and squaring off the chin, you artificially drop your visual lower third. It creates the illusion of a vertically balanced face without touching a single osteoblast.
Summary for Lazycels
- Length vs Width: Lengthening your lower third (pulling the chin down and forward) is only chemically possible at 16–18. Widening your jaw (adding masseter/gonial bone) is possible as an adult.
- The Jaw is an AR Hotbed: Mandibular bone cells house up to three times the androgen receptors of your axial skeleton. The jaw is highly reactive to hormones, but only when the biological doors are actually open.
- The Age 16–18 Window (Mandibular Lengthening): This is your only shot to gain physical mandibular length. Keep estrogen crushed to prevent fusion, and run steady-state GH (IGF-1) with a non-aromatizing androgen like Anavar to deposit new bone. Aromatizing compounds like high-dose test will instantly destroy this window.
- The Age 21+ Reality (No Extra Length): Your growth sites are mineralized. High-dose GH won't swing your jaw forward. It will just give you a swollen tongue, tooth gaps, and a Neanderthal brow ridge.
- The Age 21+ Cortical Flare Option: You can still widen the jaw laterally. Combine non-aromatizing DHT derivatives (Masteron + Primobolan) with heavy mechanical chewing and bone-mineralization cofactors (D3 + K2).
- Topical Creams are Cope: Rubbing DHT cream on your jawline just enters your bloodstream and makes you bald. It doesn't target the bone.
- Beard Frauding: If your bones are locked and you're broke, grow out the chin/jawline hair and keep the cheeks tight. It visually drops the lower third and balances your proportions instantly.
The 13-15 Pubertal Growth
Engine: Height & Lower-Third Protocols
Engine: Height & Lower-Third Protocols
Between the ages of 13 and 15, your growth plates are highly active and
incredibly responsive—both in the long bones for vertical height and the
mandibular condyles for your jaw. Capitalizing on this peak developmental window
requires maximizing systemic IGF-1 levels. Pharmaceutically, this is done by
running high-purity Recombinant Human Growth Hormone (rhGH) at 2 IU to 3 IU
daily, administered subcutaneously on an empty stomach right before sleep.
Because estrogen (E2) drives epiphyseal plate fusion and limits your growth
runway, keeping estrogen in a low-normal range is non-negotiable if you want to
delay joint mineralization. You can manage this pharmaceutically with a
micro-dose of Anastrozole (0.25 mg once or twice a week). Alternatively, you can
stack natural estrogen modulators. Start with Boron (6 mg daily) to lower SHBG,
which increases free testosterone while naturally lowering serum estradiol. Pair
this with 100 mg of DIM (Diindolylmethane) daily to shift estrogen metabolism
away from the highly active 16-alpha pathway, and add Zinc Picolinate (30 mg
daily) to act as a mild, natural aromatase inhibitor. To maximize endogenous
testosterone, introduce Tongkat Ali (200 mg daily). It stimulates luteinizing
hormone (LH) to boost Leydig cell output without shutting down your developing
HPTA, supplying the precise androgenic signaling your skeleton needs for density
and structural definition.
While systemic hormones provide the raw building blocks, mechanical forces
dictate where that new bone is actually deposited. Proper oral posture (mewing)
is vital to guide the remodeling maxilla upward and forward, preventing a
down-swung, long-face profile. To complement this, introduce progressive
mechanical loading. Chewing hard mastic gum for 20 minutes every other day
triggers mechanotransduction, signaling the mandibular condyle to remodel and
expand at the jaw joints. This dual approach leverages elevated GH and free
testosterone to widen your dental arches and project the lower third forward.
Finally, to fuel this rapid osteogenesis, support the protocol with a targeted
bone-mineralization matrix: 5,000 IU of Vitamin D3 and 5 mg of Vitamin K2 (MK-4)
daily. This specific pairing routes calcium directly into your lengthening
skeletal frame instead of soft tissues, locking in every last millimeter of
potential height and jawline projection.
To execute this protocol, bypass cheap plastic massagers and use a solid, high-density tool with sufficient mass to penetrate soft tissue and directly impact the periosteum—specifically, a polished 0.5 lb steel mallet wrapped tightly in a 1/4-inch neoprene sleeve to absorb surface-level skin trauma and prevent hematomas. Target the structural margins of the zygomatic body and the gonial angle of the mandible, completely avoiding the thin maxillary sinus walls and the infraorbital nerve. Hold the tool at a 90-degree perpendicular angle to the bone and deliver rapid, controlled, light-to-moderate taps, aiming for 50-100 repetitions per site with a frequency of every 48 hours to allow the localized inflammatory response to initiate the signaling cascade for bone deposition.
For maximum osteogenic remodeling, synchronize this mechanical stimulation with a pharmacological profile characterized by high androgen receptor saturation and low-to-moderate estrogenic activity. Apply a topical 10% DHT gel directly to the target facial areas 2 hours post-trauma, or maintain a systemic baseline using synthetic DHT derivatives like Drostanolone at 150mg/week or oral Mesterolone at 50mg/day. This hormonal environment ensures that when the damaged osteocytes downregulate sclerostin and activate the Wnt/β-catenin pathway within the 24-48 hours post-impact recovery window, the newly recruited osteoblasts are backed by maximum androgenic signaling, locking in permanent, mineralized cortical thickening while suppressing osteoclastic bone resorption.
For maximum osteogenic remodeling, synchronize this mechanical stimulation with a pharmacological profile characterized by high androgen receptor saturation and low-to-moderate estrogenic activity. Apply a topical 10% DHT gel directly to the target facial areas 2 hours post-trauma, or maintain a systemic baseline using synthetic DHT derivatives like Drostanolone at 150mg/week or oral Mesterolone at 50mg/day. This hormonal environment ensures that when the damaged osteocytes downregulate sclerostin and activate the Wnt/β-catenin pathway within the 24-48 hours post-impact recovery window, the newly recruited osteoblasts are backed by maximum androgenic signaling, locking in permanent, mineralized cortical thickening while suppressing osteoclastic bone resorption.
𝑻𝒉𝒆 𝑺𝒕𝒆𝒓𝒐𝒊𝒅 𝑻𝒊𝒎𝒊𝒏𝒈 𝑻𝒉𝒆𝒐𝒓𝒚Here is my theory on the
optimal timing for
anabolic steroid use,
specifically for
maximizing overall bone mass
and
optimizing lower-third skeletal development.
The best age to take anabolic-androgenic steroids is approximatly beetween 16.5 - 19.5 years of age and in this section i will explain why...
To the 1% of you with the focus to actually make it this far: pause. Take a deep, deliberate breath. Walk to your kitchen, pour a glass of ice water, and stand in front of the mirror. Don't scan your reflection for flaws. Look at yourself to recognize the face and body of the person you are actively architecting.
ok back to topic
◆ Why Exactly in This 36-Month Window? ◆
If you're looking for sources for prescription drugs, peptides, or steroids,The human skeleton develops via two distinct biological pathways: endochondral
ossification (driving long bone growth and height) and intramembranous
ossification (building the cranial vault and facial bones).
Epiphyseal growth plates in the appendicular skeleton—specifically the femur and
tibia—are exquisitely sensitive to Estradiol (E2). Estrogen receptor alpha (ERα)
activation is the exact biological switch that drives plate senescence and
permanent fusion. This creates a brutal physiological trap. If a 14-year-old
pins exogenous Testosterone Enanthate, the aromatase enzyme rapidly converts
that massive androgenic surplus directly into E2. The consequence is immediate
and irreversible: his long bones fuse within months. He stays 5'6" for the rest
of his life. In the real world, that is aesthetic suicide.
By age 16.5, the average male has reached 95% of his terminal adult height. The
growth plates in the long bones are either actively narrowing or completely
sealed. With linear growth practically finished, the risk of permanently
stunting your vertical frame drops to near zero.
You might argue that blasting androgens at 14 to 16 yields mathematically
superior facial bone structure. Technically, you are correct. That earlier
bracket is structurally superior for one specific reason: the cranial base
remains highly plastic.
During this earlier window, the spheno-occipital synchondrosis (SOS)—the central
growth cartilage located behind the midface—is actively proliferating.
Cephalometric data confirms that high androgen exposure at 14 or 15 translates
the maxilla completely forward. It expands the SNA angle, delivering a flawless
forward growth vector. You are shifting the actual spatial coordinates of the
skull.
But there is a massive catch.
To capitalize on that 14–16 facial plasticity without nuking your height, you
have to execute a flawless pharmacological protocol. You must constantly pull
bloodwork and meticulously titrate an aromatase inhibitor (like Exemestane) to
keep your Estradiol perfectly suppressed. If your E2 spikes, your long bones
fuse instantly. If you crash your E2 to zero, osteoblast proliferation halts,
bone mineral density collapses, and the midface stops moving entirely.
It is a tightrope walk over razor wire. The vast majority of teenagers lack the
bloodwork access, discipline, and capital to pull it off. They walk away with a
decent jawline on a 5'6" frame—a definitively terrible trade.
◆ The 16.5 - 19.5 Solution: Periosteal Overdrive ◆
This is why the 16.5 to 19.5 window takes the throne. It represents the ultimate
intersection of risk mitigation and aesthetic payoff.
By 16.5, the height equation is solved. The tibial and femoral epiphyses are
sealing. Introduce a heavy androgenic load at this precise stage, and the
biological machinery shifts its physiological priority. Since the skeleton can
no longer grow longer (endochondral translation), the mechanical target switches
entirely to intramembranous and periosteal ossification.
The bones grow thicker.
Time your androgen exposure within this specific 36-month block, and you bypass
the E2 height-trap entirely, directly stimulating three highly specific
aesthetic vectors:
1. The Gonial Flare (Lower-Third Expansion) The masseteric insertion points at
the corners of your mandible are densely packed with androgen receptors.
Flooding these receptors between 16.5 and 19 triggers severe, localized
appositional bone growth. Your jaw does not necessarily move further
forward; instead, it flares laterally. This mechanical loading thickens the
rami, delivering the wide bi-gonial width that defines the modern
lower-third ideal.
2. Supraorbital Torus Thickening Dihydrotestosterone (DHT) acts aggressively on
the brow ridge during late adolescence. Periosteal apposition here
physically deepens the orbits. You build a thicker shelf of bone that
structurally shields the eyes, creating a deep-set, hooded aesthetic purely
through skeletal accumulation.
3. The Acromioclavicular Vector While your legs stop growing around 17, your
medial clavicular epiphyses remain wide open—often until age 22. Running
androgens in this specific window allows you to aggressively widen your
bideltoid breadth, expanding your skeletal frame and cementing a dominant
shoulder-to-waist ratio.
these are a few options worth checking out:
VETTED
PROCUREMENT DIRECTORY No-nonsense evaluation of peptide, androgen,
and prescription sources.
─────────────────────────────────────────────────────
PROCUREMENT DIRECTORY No-nonsense evaluation of peptide, androgen,
and prescription sources.
─────────────────────────────────────────────────────
█ HIGH TIER / FULLY LEGIT[/B>
Verified Peptides
https://verifiedpeptides.com/product/bpc-157-tb-500-blend/
• Category: Peptides (BPC-157, TB-500, GHK-Cu) • Quality: High
(Third-party verified) • Pricing: Standard Retail • Verdict: The
gold standard for domestic peps. If you're prioritizing purity for injury
recovery or skinmaxxing and don't want to gamble with your health, start here.
Deus Power https://deuspower.shop/ •
Category: Androgens, PCT, HGH, SARMs • Quality: Very High
(Authorized Deus Medical reseller) • Pricing: Competitive •
Verdict: Top-tier reliability. Deus is widely regarded as one of the best
EU labs on the forum. Shipping is discreet—usually disguised as vitamins or
cosmetic oils—making them the premier choice for EU/UK buyers.
Driada Medical https://driadashop.to/
• Category: Androgens, HGH, PCT, SARMs • Quality: Very High
(Lab-tested / smooth carrier oils) • Pricing: Standard Retail •
Verdict: A dominant EU-domestic heavyweight that easily rivals Deus. They
are highly praised on Meso-Rx for their strict testing transparency and
exceptionally smooth carrier oils (primarily sesame, keeping PIP non-existent).
Just watch out for fake clone domains (like shopdriada.eu)—only order from the
official .to site.
Steroidify
https://www.steroidify.ltd/Trenbolone
• Category: Androgens, PCT, Ancillaries • Quality: High /
Brand-dependent (Stocks official Deus, Pharmacom, etc.) • Pricing:
Premium • Verdict: The "concierge" option. You're paying a convenience
markup, but the professional customer service, delivery guarantees, and payment
flexibility are unmatched in this space.
─────────────────────────────────────────────────────
█ MID TIER / SITUATIONAL[/B>
TheBBPower https://thebbpower.com/ •
Category: AAS, HGH, PCT • Quality: Solid (Official Hilma Biocare
distributor) • Pricing: Standard UGL • Verdict: A dedicated EU
domestic source heavily pushing Hilma Biocare. Vouched for on MesoRX as a
reliable European option, but proceed with caution—enough scattered complaints
exist regarding slow shipping and dropped communications on secondary boards to
warrant a test order first. Viable, but Deus Power remains the superior EU
route.
Iron Lion Lab
https://ironlion-lab.is/shop/ •
Category: HGH, Peptides, AAS • Quality: Reliable (Well-reviewed
across major boards) • Pricing: Extremely Cheap (Lowest cost-per-IU on
HGH) • Verdict: The budget king for heightmaxxing runs via Puretropin.
The gear is solid, but shipping can be an absolute nightmare. Order weeks in
advance or prepare to wait.
UK-Peptides
https://www.uk-peptides.com/ •
Category: Peptides • Quality: Consistent • Pricing:
Standard • Verdict: The safest bet for UK/EU buyers who want fast
shipping and zero customs anxiety.
AllDayChemist
https://www.alldaychemist.com/ •
Category: Prescription Drugs (Accutane, Aromasin, Hair Loss, PCT) •
Quality: Pharma-Grade (Generic Indian pharma) • Pricing: Cheap •
Verdict: An industry veteran. The go-to for cheap Accutane, Finasteride,
or Dutasteride. While the purity is pharmaceutical standard, be prepared for a
clunky payment process and shipping that takes weeks.
─────────────────────────────────────────────────────
█ OVERPRICED / AVOID[/B>
MisteRoid Pharma
https://misteroidpharma.site/shop/
• Category: AAS / Underground Lab • Quality: Highly Suspect
(Unverified / Shilled) • Pricing: Honeypot • Verdict: Hard pass.
Major red flags across the board. Forum veterans recently exposed their rep on
Eroids for allegedly spinning up dummy accounts to spam five-star reviews on
their own gear. Don't risk injecting unverified bathtub oil when established,
top-tier labs are readily available.
Enhanced Labs
https://enhancedlabs.com/collections/all
• Category: SARMs, Supplements • Quality: Average •
Pricing: Overpriced • Verdict: Influencer bait. The products work,
but you're paying a massive premium to fund their marketing budget. Skip the
hype and buy from specialized labs.
IndiaMart http://www.indiamart.com
• Category: Industrial Bulk Raw Powders • Quality: High Risk
(Unregulated) • Pricing: Wholesale Floor • Verdict: This is a B2B
industrial site, not a retail shop. Buying small batches here is a gamble with
heavy metal contamination and underdosing. Unless you're an experienced chemist
with your own HPLC testing equipment, stay away.
─────────────────────────────────────────────────────
BODY
FAT
&
JAWLINE
DEFINITION
The Soft Tissue Drape • The Limits of Fat Loss • Neck Definition
First, let's determine the ideal body fat percentage for bone definition and clarity in the lower third. Before we go any further, we first need to understand what body fat actually is.
━━━━━━━━━━
❖ WHAT IS BODY FAT? ❖ ━━━━━━━━━━At its core, body fat is
triglycerides stored within adipocytes. Aesthetically, this subcutaneous adipose
tissue acts as a biological blur filter over your musculoskeletal
frame.
⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯
When your body fat percentage is high, this subcutaneous
layer thickens. It fills in natural facial depressions—like the submalar
space—and rounds out sharp skeletal landmarks. This masks muscle belly
separation and buries the defining contours of the skull, specifically the
zygomatic arch, the mandibular border, and the gonial angle.
⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯
As you lean out and those adipocytes shrink, this
overlying layer thins. The skin and superficial fascia drape tightly against the
underlying bone and muscle. That dramatic shift from a "soft" face to a
"chiseled" one isn't the result of your skeletal structure changing overnight.
It is the physical decompression of the tissue, letting the hard edges of your
skull dictate how light and shadow hit your
face.
The Paradigm of Body Fat and Bone Definition
Summary for Neurodivergent/Smooth-Brained people:
To carve out peak skeletal and muscle definition, 9% body fat is the
absolute gold standard.
The Skeletal Definition Equilibrium
Theory
◆ ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
◆
Facial definition is fundamentally an optical game of
contrast, governed by how cleanly light breaks across the underlying bone
structure. In a high-adipose state, the superficial subcutaneous fat acts as a
physical diffuser. It takes high-contrast skeletal landmarks—specifically
the zygomatic arches, the mandibular border, and the gonial angles—and
rounds them off under a soft, non-reflective layer. This loss of angularity is
not a structural bone deficiency, but an optical occlusion; the fat
simply scatters the light, erasing the sharp transitions between facial planes.
❖
Maximizing this definition requires a systematic reduction of this
diffusion layer to alter the drape of the skin. As superficial fat thins, the
skin conforms tightly to the underlying craniofacial architecture. The result is
a sharp, geometric interplay of light and shadow, creating
three-dimensional depth and maximizing visual contrast without requiring
invasive bony augmentation.
❖
The upper limit of this optical optimization is governed by a strict
biological trade-off between two distinct fat compartments:
superficial and deep. While stripping the superficial layer reveals bone,
depleting the deep fat compartments (such as the buccal and deep malar
pads) collapses the midface. Without these deep structural pillars, the face
loses its youthful fullness, transitions become gaunt rather than sharp,
and the soft-tissue envelope looks deflated.
❖
The skeletal definition equilibrium represents the exact mathematical
point where superficial adipose is sufficiently minimized to maximize shadow
casting, yet deep structural fat remains intact to support facial harmony. For
the male craniofacial structure, this physical optimization point resolves at
approximately 9% body fat. It is the absolute
threshold where the jawline and cheekbones achieve maximum angular
contrast before the midface begins to collapse into aesthetic decay.
I AM NOT WRITING A GUIDE TO LOSE BODY FAT THIS SHOULD BE SELF-EXPLANATORY. For P.E.D.S, to reduce BF%; Ages 13-18.
The Protocol:
Run this for 6-8 weeks max. You must be in a strict
caloric deficit.
GW-501516
(Cardarine): 10mg - 15mg / day
(Dosed 45 mins pre-workout).
Mechanism: PPARδ agonist. Shifts your
body's energy preference from glycolysis to lipid oxidation. Significantly
increases AMP-activated protein kinase (AMPK) expression.
Rauwolscine (Alpha-Yohimbine):
1.5mg - 3mg / day (Taken
strictly upon waking, fasted, before morning cardio).
Mechanism: Alpha-2 adrenoceptor
antagonist. Stubborn lower-ab fat cells are packed with alpha-2 receptors that
actively halt lipolysis. This compound blocks them, allowing catecholamines to
burn the fat. Do not consume with carbs; an insulin spike renders it
biologically useless.
MK-677 (Ibutamoren) - If you insist on
using it to heightmaxx simultaneously: 10mg / day
(Strictly dosed right before bed).
Mechanism: GH secretagogue. Taking it at
night lets you sleep through the extreme hunger pulses. The GH spike preserves
muscle tissue in a deep deficit, but you will hold water. Drop the MK-677
exactly 10-14 days before you want to actually see your 9% physique so your body
drops the extracellular bloat.
Why did this section turn out like
such absolute garbage? Honestly, whatever. I'm over it, fuckass im not re-doing
this.
We’ve locked in the two highest-ROI structural shifts: lower-third development and skeletal definition.
Now, the focus turns to the high-yield softmaxes that tie the entire look together.
The Definitive Lower Third SoftmaxxingCompendium
A Complete Anatomical Guide to Non-Surgical Mandibular, Masseter, and
Mentalis Optimization
Note: Softmaxxing, will include Performance Enhancing drugs, although no surgery
The Teen Jaw-Growth Protocol
Step-by-Step Daily Routine
Step-by-Step Daily Routine
Step 1: The Masticatory Load Protocol
(Masseter Hypertrophy & Condyle Remodeling)
Stop wasting money on cheap, soft chewing gum. It dissolves in minutes and simply does not provide the mechanical resistance required to trigger actual bone remodeling.
Material:
You need 100% natural mastic gum or high-resistance Falim gum. If you don't want to chew gum, force tough, heavily dehydrated foods into your diet—think biltong, thick cuts of tough meat, or raw carrots.
Routine:
Chew for 20 to 30 minutes every other day. Do not push past the 30-minute mark; overloading the joint just leads to TMJ inflammation, which will set your progress back.
Technique:
Only chew on your molars, and alternate sides with every bite to keep your facial development symmetrical. Keep your lips sealed shut. Crucially, do not use your cheeks (buccinator muscles) to move the gum around. Use your tongue. Relying on your cheeks will bloat your face, whereas tongue-driven chewing keeps the cheeks flat and hollow.
Step 2: Nighttime Airway Stabilization
(Mouth Taping)
Growth happens while you sleep. If you mouth-breathe at night, your jaw drops open, forcing a clockwise, downward growth pattern that ruins facial projection.
Material:
Get 3M Micropore medical tape. It does the job without ripping your skin off in the morning.
Routine:
Place a small vertical strip right over the center of your lips before bed. This physically forces nasal breathing throughout the night.
Prerequisite:
This only works if your nasal airway is actually clear. If you suffer from chronic allergies, hit your nose with a saline spray or throw on a nasal dilator strip first. Never tape your mouth shut if your nose is completely blocked.
Step 3: The Myofunctional Swallow
(Dynamic Tongue Posture)
Static "mewing" is practically useless if you still have an infantile swallow pattern. Infantile swallowing relies on the buccinator muscles to force food down. That pushes the dental arch inward while blowing out your cheeks, giving you a permanently bloated look.
Exercise:
The "Mona Lisa" Swallow.
Method:
Gather some saliva on top of your tongue. Pin the tip of your tongue against the alveolar ridge—that little bump just behind your front teeth—making sure you aren't actually touching the teeth themselves. Now press the entire body of your tongue, especially the posterior third, completely flat against the roof of your mouth. Swallow. Do it without moving your lips, your cheeks, or your neck muscles.
Frequency:
Force yourself to do this every single time you eat or drink. Eventually, this conscious mechanical effort rewires into your subconscious default swallow. When that happens, you start applying heavy forward and lateral force to your maxilla thousands of times a day.
Step 4: The Pharmacological Matrix
(Endocrine Puberty-Maxxing)
Chewing provides mechanical stress, which locally upregulates the Wnt/β-catenin pathway. However, systemic IGF-1 dictates the actual raw materials available for bone apposition. The strategy here is straightforward: spike your growth factors while simultaneously delaying growth plate fusion.
Compound A: MK-677 (Ibutamoren) - GH/IGF-1 Secretagogue
Mechanism:
MK-677 binds to the ghrelin receptor, commanding the pituitary gland to release massive pulses of endogenous HGH. This triggers a drastic elevation in systemic IGF-1, forcing your condylar cartilage into rapid proliferation right before endochondral ossification locks it in.
Theoretical Dose:
12.5mg orally, taken strictly before bed.
Tradeoffs & Coping:
Be warned: MK-677 drives up insulin resistance and causes heavy water retention. You will probably get "moon face" and look bloated during the cycle. That is the temporary tradeoff for permanent bone density. You have to monitor your fasting blood glucose. Cycle the compound (for example, 5 days on, 2 days off) so you don't permanently desensitize your pituitary gland.
Compound B: Exemestane (Aromasin) - Suicidal Aromatase Inhibitor
Mechanism:
Exemestane binds irreversibly to the aromatase enzyme. This shuts down the conversion of testosterone into estradiol (E2). Since high E2 is the exact signal that tells your body to calcify and fuse its growth plates, micro-dosing an AI artificially keeps that pubertal growth window open—buying you months, and sometimes years, of extra development.
Theoretical Dose:
6.25mg orally, taken every 3.5 days (twice a week).
Tradeoffs & Coping:
Do not completely nuke your E2. Flatlining your estrogen leads to severe joint desiccation (which means brutal TMJ pain when you chew), osteopenia, and heavy cognitive brain fog. The objective is to push E2 down into the low-normal reference range, not crash it to zero. Exemestane is the drug of choice over Arimidex because it prevents massive estrogen rebound the second you halt the cycle.
The Teen Jaw-Growth Protocol
Clinical Overview
Targeting teenagers aged 14 to 19 before their growth plates fuse, this protocol
merges masticatory biomechanics with endocrine modulation to actively maximize
lower facial bone development. While the regimen carries side effects like TMJ
inflammation, insulin resistance, and estrogen depletion, these metabolic and
structural threats can be systematically neutralized through disciplined drug
cycling, exact dose titration, and strict adherence to the mechanical
thresholds.
Puberty Protocol (Under 18): Sutural Malleability & Mandibular Redirection
At this age, your spheno-occipital synchondrosis and midfacial sutures haven't fully fused. This leaves a brief biological window for actual bone redirection—the primary factor dictating the length of your submental plane.
1. The Somatic Swallow Overlay
Most people with a poor cervicomental angle (CMA) rely on a retained visceral swallow, engaging the buccinators and perioral muscles. This pulls the mandible down and backward during the roughly 2,000 swallows you perform every day.
The Fix:
You need to transition to a somatic swallow. Lock the tip of your tongue against the incisive papilla, using the posterior third to create a vacuum against the soft palate.
The Mechanism:
This creates negative intraoral pressure. Applied consistently over the years of puberty, this continuous upward and forward vector physically guides the translation of the maxilla and mandible. It lengthens the jawline and pulls the neck skin taut across your developing bone structure.
2. Hyoid Bone Anchoring
Your hyoid bone remains highly mobile throughout puberty.
The Fix:
Keep the styloglossus and hyoglossus muscles constantly engaged by holding the posterior third of your tongue elevated.
The Mechanism:
These muscles connect the tongue directly to the hyoid bone. When held in a shortened, flexed position around the clock, fascial remodeling kicks in. As you grow, the body physically shortens these tissues, permanently anchoring the hyoid bone higher up (closer to C3) to carve out a sharp 105-degree angle.
21+ Protocol: Adult Neuromuscular & Fascial Remodeling
Past the age of 21, your craniofacial skeleton is fully fused. At this point, the bone isn't moving without a saw. Your entire focus must shift to shortening the resting length of the suprahyoid muscles and aggressively tightening the deep cervical fascia.
1. Mylohyoid Isometric Shortening
The mylohyoid forms the muscular floor of your mouth. When weak, it droops like a hammock and ruins your CMA.
The Protocol:
Execute max-force isometric tongue presses. Flatten your entire tongue against the roof of the mouth and press upward with 80–90% of your maximum force for a 60-second hold. Repeat this 10 times a day.
The Mechanism:
This induces adaptive shortening of both the mylohyoid and geniohyoid. By repeatedly forcing these muscles into maximum isometric contraction while fully shortened, you rewire their neuromuscular resting tone. They eventually learn to sit higher at rest, pulling the submental skin up with them.
2. Digastric Muscle Atrophy via Agonist Overload
A bulky anterior digastric belly creates a distinct bulge right beneath the chin.
The Protocol:
Stop chewing large boluses of tough food or mastic gum with an open mouth or exaggerated lateral jaw movements.
The Mechanism:
The digastric muscle operates to open the jaw and depress the mandible. Chronic over-chewers frequently hypertrophy the anterior belly of the digastric, completely wrecking their CMA. By keeping your teeth in light contact and forcing the masseters to handle the workload, you trigger disuse atrophy in the anterior digastric, shrinking the submental bulge.
3. Deep Cervical Fascia Stretching
The Protocol:
Combine McKenzie chin tucks with extreme cervical extension. Retract your mandible fully, tilt your head backward to face the ceiling, and thrust your lower jaw forward into a severe underbite. Hold this position for 30 seconds.
The Mechanism:
This is not a posture drill. This movement stretches the superficial musculoaponeurotic system (SMAS) and the platysma to their absolute mechanical limits. Done consistently, it triggers localized fibroblast activity within the fascia, causing the tissue to rebound and sit much tighter against the throat cartilage.
The Holy Grail of Softmaxxing
Optimizing the Lower Third: Soft Tissue Refinement & Facial Definition
Every inch of your jawbone is wrapped in the periosteum—a dense, highly reactive fibrous membrane. Subject the mandible to extreme mechanical stress, and
osteocytes buried deep within the bone matrix immediately detect the strain.
Yet, you inevitably hit a biological brick wall: Sclerostin.
Secreted directly by your osteocytes, this glycoprotein acts as an emergency brake on skeletal expansion. It completely paralyzes the Wnt/β-catenin signaling pathway, the precise molecular cascade responsible for laying down fresh bone.
Why? Because dense cortical bone requires immense metabolic energy, and your system is hardwired to fiercely resist building it.
Attempt to brute-force the issue by aggressively chewing hard food, and your body retaliates by dumping a flood of Sclerostin into the matrix.
The result?
You build massive, puffy masseter muscles that sit uselessly on top of the exact same narrow skeletal base. If you want true, bone-deep lateral flare, you must
biochemically crush local Sclerostin expression while simultaneously flooding the masseteric tuberosity with non-aromatizing androgens.
Standard
"just take steroids" advice fails here. High-dose systemic androgens readily
aromatize into estradiol (E2), signaling rapid long-bone fusion while triggering
subcutaneous water retention that completely erases jawline definition.
To bypass Sclerostin, we hijack the parathyroid pathway.
"Intermittent administration of Parathyroid Hormone (PTH 1-34) strongly
suppresses sclerostin expression in osteocytes, leading to massive upregulation
of Wnt signaling and subsequent periosteal bone apposition." (Bellido et
al., 2013)
While continuous PTH exposure actually triggers bone resorption, micro-dosed,
intermittent PTH (Teriparatide) operates as a violently anabolic agent for
cortical bone.
There is a catch: you cannot run Teriparatide in isolation. PTH aggressively
upregulates RANKL, massively stimulating osteoclasts (the cells that devour
bone). If you pin Teriparatide and execute extreme isometric jaw clenching
without an anti-resorptive anchor, you will literally dissolve your own cortical
plates. You must pair it with a bisphosphonate to force apoptosis in those
osteoclasts.
"just take steroids" advice fails here. High-dose systemic androgens readily
aromatize into estradiol (E2), signaling rapid long-bone fusion while triggering
subcutaneous water retention that completely erases jawline definition.
To bypass Sclerostin, we hijack the parathyroid pathway.
"Intermittent administration of Parathyroid Hormone (PTH 1-34) strongly
suppresses sclerostin expression in osteocytes, leading to massive upregulation
of Wnt signaling and subsequent periosteal bone apposition." (Bellido et
al., 2013)
While continuous PTH exposure actually triggers bone resorption, micro-dosed,
intermittent PTH (Teriparatide) operates as a violently anabolic agent for
cortical bone.
There is a catch: you cannot run Teriparatide in isolation. PTH aggressively
upregulates RANKL, massively stimulating osteoclasts (the cells that devour
bone). If you pin Teriparatide and execute extreme isometric jaw clenching
without an anti-resorptive anchor, you will literally dissolve your own cortical
plates. You must pair it with a bisphosphonate to force apoptosis in those
osteoclasts.
Phase I: Transverse Width (The Cortical Flare Matrix)
You cannot systemic-maxx your way to a wider jaw without destroying your organs
or mutating into a neanderthal. The strategy requires pinning the anabolic
signaling directly to the gonial angles.
Relying on DMSO as a carrier is biomechanical suicide. Because DMSO acts as a
universal penetrant, it instantly breaches the subdermal capillary networks and
flushes the DHT straight into systemic circulation—nuking your hairline and
swelling your prostate. To keep the androgen payload physically locked at the
periosteum, you need a liposomal encapsulation base.
Objective: Strike the
high-density androgen receptors localized exactly at the gonial angles,
completely bypassing heavy hepatic first-pass metabolism.
Step 1: Secure 5g of raw Dihydrotestosterone (Stanolone) powder. Absolutely no
esterified injectables. Step 2: Dissolve the raw powder entirely into 10mL of
Propylene Glycol. Step 3: Apply gentle heat (40°C) until the solution runs
completely clear. Step 4: Suspend this mixture inside 40g of Phosphatidylcholine
(Lecithin). Step 5: Submerge it in an ultrasonic cleaner (sonicator) at 40kHz
for exactly 20 minutes to force the liposomal encapsulation.
The Application Protocol: Using a glass dropper, apply 1mL directly to the skin
over each gonial angle (the rear corners of the jaw) and firmly rub it in.
Timing: Execute this immediately post-mastication. While the liposomes easily
bypass the epidermis, their molecular size prevents them from washing into the
capillary beds. This traps the DHT payload directly in the deep fascial layers
above the bone, saturating the exact zone where your osteoblasts are currently
active.
high-density androgen receptors localized exactly at the gonial angles,
completely bypassing heavy hepatic first-pass metabolism.
Step 1: Secure 5g of raw Dihydrotestosterone (Stanolone) powder. Absolutely no
esterified injectables. Step 2: Dissolve the raw powder entirely into 10mL of
Propylene Glycol. Step 3: Apply gentle heat (40°C) until the solution runs
completely clear. Step 4: Suspend this mixture inside 40g of Phosphatidylcholine
(Lecithin). Step 5: Submerge it in an ultrasonic cleaner (sonicator) at 40kHz
for exactly 20 minutes to force the liposomal encapsulation.
The Application Protocol: Using a glass dropper, apply 1mL directly to the skin
over each gonial angle (the rear corners of the jaw) and firmly rub it in.
Timing: Execute this immediately post-mastication. While the liposomes easily
bypass the epidermis, their molecular size prevents them from washing into the
capillary beds. This traps the DHT payload directly in the deep fascial layers
above the bone, saturating the exact zone where your osteoblasts are currently
active.
Phase II: The Mechanical & Systemic Trigger
With the DHT locally pooled at the jawbone, you now have to force the actual
calcification.
1. The Sclerostin-Killer Stack: Administer 20mcg of Teriparatide (Forteo)
subcutaneously into the abdomen every morning. Alongside this, take 70mg of
Alendronate (a potent bisphosphonate) orally once a week. The Teriparatide
crushes local Sclerostin expression, giving the osteoblasts the green light
to construct new bone. Meanwhile, the Alendronate chemically paralyzes the
osteoclasts, ensuring that the newly formed matrix isn't instantly
reabsorbed. Cap this cycle at a strict 12-week maximum to mitigate any
osteosarcoma risks.
2. High-Density Isometrics (Stop Chewing): Endless dynamic chewing builds the
wrong muscle fibers (Type I), yielding a bulky, soft-looking masseter
profile. The objective is localized bone strain, not muscular hypertrophy.
Position a dense silicone block squarely between your rear molars. Bite down
at 90% of your absolute maximum force and hold that brutal static isometric
contraction for 45 seconds. Execute 5 sets per side, strictly every other day.
This extreme static load physically bends the mandible at a microscopic level,
generating the exact piezoelectric charge required to pull calcium directly into
the hydroxyapatite matrix.
Phase III: Sagittal Projection (Submental Fibrosis)
Once your skeletal structure fuses, your side profile is dictated by a single
variable: how tightly the soft tissue wraps beneath the mandible. If your hyoid
bone rests low, you are stuck with a permanent double chin.
Pumping the area full of fat-burners like Kybella simply destroys the adipose
tissue, leaving you with empty, loose skin draping off a recessed jaw. Instead,
the strategy is to intentionally induce localized scarring (fibrosis) to
physically shrink-wrap the submental fascia.
Prostaglandin F2-alpha (PGF2a)
is an intensely inflammatory lipid compound, traditionally leveraged in extreme
bodybuilding for localized muscle site-enhancement.
Micro-dosed directly into the submental fat pad and the platysma muscle, PGF2a
sparks extreme, highly localized inflammation. As the damaged tissue heals,
fibroblasts deposit dense webs of Type-I collagen, effectively forging internal
scar tissue. This calculated fibrotic response physically contracts the fascia,
pulling the surrounding skin brutally flat against the underside of the
mandible.
The Execution: Because PGF2a operates on a half-life measured in mere minutes, a
once-a-week injection schedule is biologically useless. You must sustain the
macrophage response.
Using a 30G 1/2" insulin pin, map out a strict grid of 4 injection sites
directly beneath the chin (targeting the submental triangle). Inject
exactly 0.1mg of PGF2a per site every 12 hours for 14 continuous days.
Expect the inflammation to be profound—for a brief period, you will look like a
pelican. But as the severe swelling clears over the following two weeks, the
submental fascia will violently tighten, permanently shrink-wrapping the tissue
to artificially carve out a razor-sharp mentocervical angle.
is an intensely inflammatory lipid compound, traditionally leveraged in extreme
bodybuilding for localized muscle site-enhancement.
Micro-dosed directly into the submental fat pad and the platysma muscle, PGF2a
sparks extreme, highly localized inflammation. As the damaged tissue heals,
fibroblasts deposit dense webs of Type-I collagen, effectively forging internal
scar tissue. This calculated fibrotic response physically contracts the fascia,
pulling the surrounding skin brutally flat against the underside of the
mandible.
The Execution: Because PGF2a operates on a half-life measured in mere minutes, a
once-a-week injection schedule is biologically useless. You must sustain the
macrophage response.
Using a 30G 1/2" insulin pin, map out a strict grid of 4 injection sites
directly beneath the chin (targeting the submental triangle). Inject
exactly 0.1mg of PGF2a per site every 12 hours for 14 continuous days.
Expect the inflammation to be profound—for a brief period, you will look like a
pelican. But as the severe swelling clears over the following two weeks, the
submental fascia will violently tighten, permanently shrink-wrapping the tissue
to artificially carve out a razor-sharp mentocervical angle.
This is meant to produce a rip-off of a surgery such as trimax, although the results will defentiely be a lot diffrent.
also a risk of bone cancer, but liitle.
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Transition
Transition
We have already covered how DHT and specific pathways influence the mandible,
detailing the mechanics of bone growth and every effective PED for the lower
third.
Now, it is time to shift focus.
This next topic completely bypasses your
genetic baseline.
Rather than simply optimizing the skeletal structure you
already have, this method allows you to generate entirely new bone and
physically reposition it; Hardmaxxing
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
THE LOWER THIRD
Anatomical Reconstruction & Hardmaxxing Protocol
BIMAX • GENIOPLASTY • CUSTOM IMPLANTS • GONIAL ANGLES
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
The hardmaxxing guide is too long to fit in a single thread, so I'm giving it its own post and will link it here.THE LOWER THIRD
Anatomical Reconstruction & Hardmaxxing Protocol
BIMAX • GENIOPLASTY • CUSTOM IMPLANTS • GONIAL ANGLES
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Link: https://looksmax.org/threads/hardmaxxing-lower-third.2228707/