D
Deleted member 80642
ChadLite2027
- Joined
- Jul 9, 2024
- Posts
- 1,986
- Reputation
- 3,183
Many of you have probably seen my thread:

 looksmax.org
looksmax.org
And noticed that I had decent results, so naturally want a similar surgical outcome.
However, many people also may not understand the use of these surgeries, specifically Ptosis Repair, and who is indicated for it.
In this short thread I will explain who is and isn't indicated for ptosis repair
Firstly here is someone who HAS upper eyelid exposure, but is still not indicated for Ptosis repair.

As you can see he clearly has some UEE, but ptosis repair in this case would not give an aesthetic benefit. It would only risk overcorrecting and making you not be able to close eyes properly. Hardly any of the upper eyelid is covering any of the iris, and none of the pupil.
Next we have someone who is CLINICALLY indicated for ptosis repair surgery:

As you can see the eyelids are sagging far down enough that it is covering a significant amount of the iris, and even part of the pupils. This is where, if causing eyesight issues, you could get this surgery medically covered.
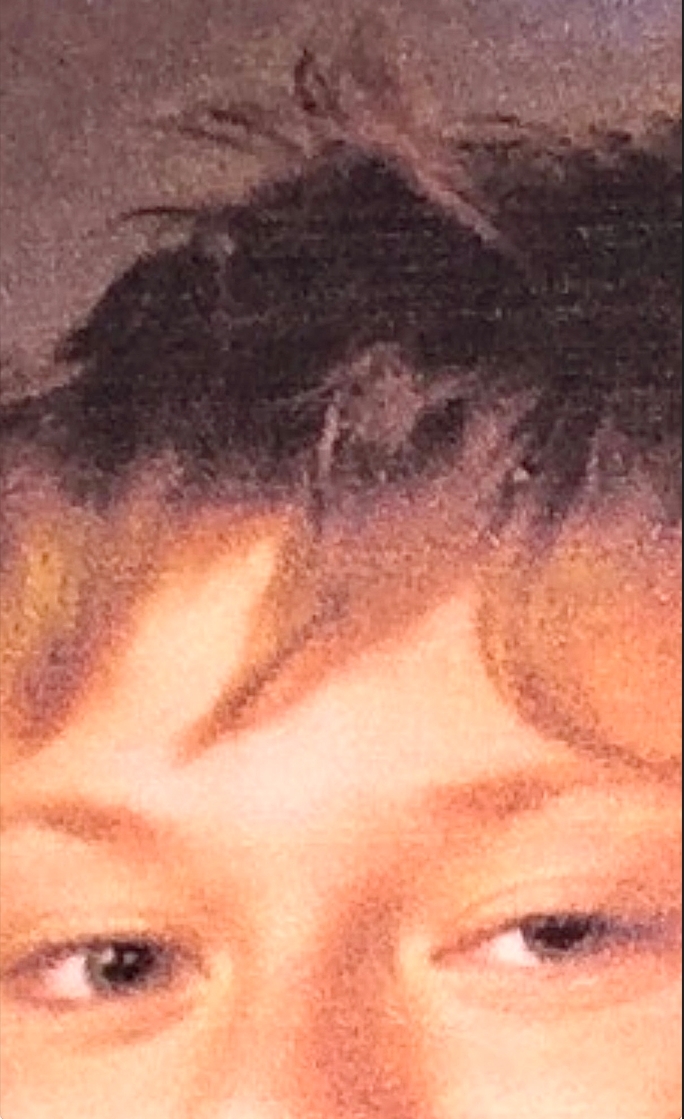
And finally you have my case, someone who is NOT medically/clinically indicated for Ptosis Repair surgery, but would benefit aesthetically from it.

Image quality is not ideal, but there is no part of the upper eyelid that would sag far down enough to cover my pupils, but enough to have a semi significant amount covering the iris.
So it is important to figure out which one you are. To see whether you are indicated for this surgery or not.
@yussimania
@lurking truecel
@LEFORT17
@DnrGriffith
@cortisolman2
FAT GRAFTING TO ORBITALS RESULTS
I am making this thread because too many people keep messaging me about my results. I am now 4.5 months post op. Bear in mind I got the surgery at 18, which is not allowed without parental consent in the country I got this done in. So I had to fake my parents e- signature to get this done. The...
looksmax.org
And noticed that I had decent results, so naturally want a similar surgical outcome.
However, many people also may not understand the use of these surgeries, specifically Ptosis Repair, and who is indicated for it.
In this short thread I will explain who is and isn't indicated for ptosis repair
Firstly here is someone who HAS upper eyelid exposure, but is still not indicated for Ptosis repair.

As you can see he clearly has some UEE, but ptosis repair in this case would not give an aesthetic benefit. It would only risk overcorrecting and making you not be able to close eyes properly. Hardly any of the upper eyelid is covering any of the iris, and none of the pupil.
Next we have someone who is CLINICALLY indicated for ptosis repair surgery:

As you can see the eyelids are sagging far down enough that it is covering a significant amount of the iris, and even part of the pupils. This is where, if causing eyesight issues, you could get this surgery medically covered.
And finally you have my case, someone who is NOT medically/clinically indicated for Ptosis Repair surgery, but would benefit aesthetically from it.

Image quality is not ideal, but there is no part of the upper eyelid that would sag far down enough to cover my pupils, but enough to have a semi significant amount covering the iris.
So it is important to figure out which one you are. To see whether you are indicated for this surgery or not.
@yussimania
@lurking truecel
@LEFORT17
@DnrGriffith
@cortisolman2