





FTWCHRVS
Iron
- Joined
- Mar 15, 2026
- Posts
- 6
- Reputation
- 4
ATCHLIST +
Every Natural & Superficial Method to Maximize Bone Density, Thickness & Architecture

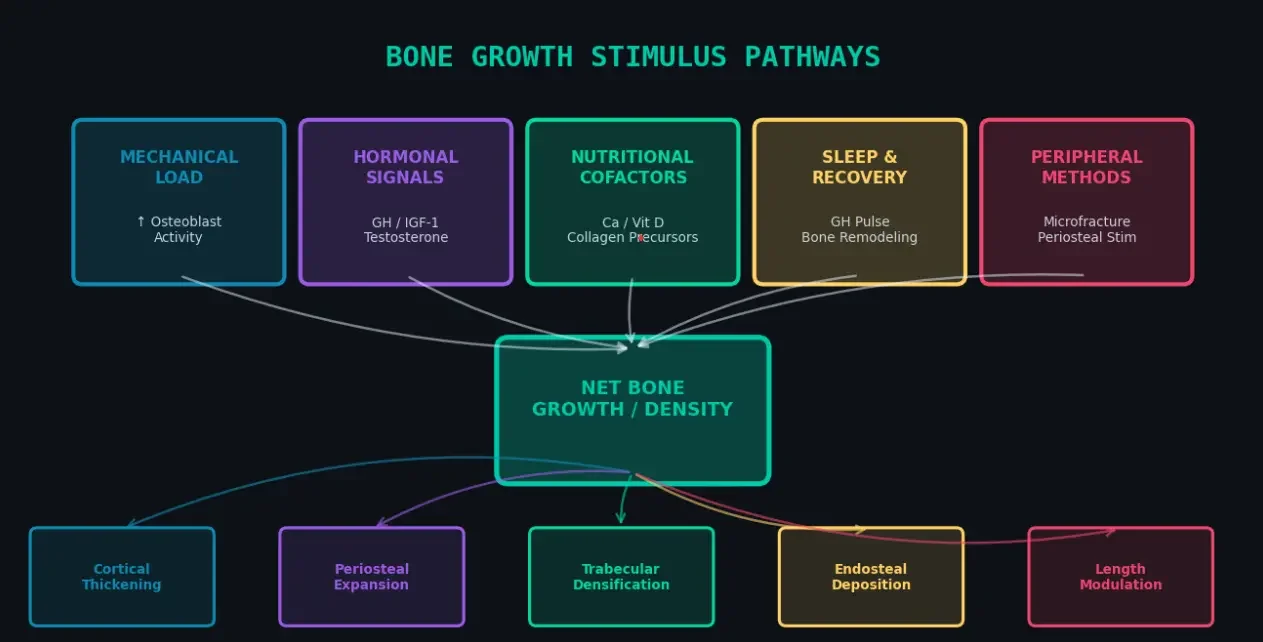
igure 1 — The five major input pathways that converge to drive net bone growth, and the five structural outcomes they produce.
Bone is a dynamic, metabolically active tissue undergoing constant remodeling. Understanding what can be influenced andwhat cannot is the foundation of any effective protocol
StructureWhat It IsCan It Grow?Primary StimulusPeriosteumFibrous membrane wrapping bone outer surfaceYES outer diameterCompressive/tensile mechanical loadCortical (compact)Dense outer shell; ~80% of bone massYES thicknessHigh-impact loading, androgensTrabecular (cancellous)Inner spongy lattice at epiphysesYES density/architecture Impacttecture Impact + nutrition + hormonesEndosteumInner surface lining medullary cavitYES variableHormonal signaling (PTH, estrogen)Epiphyseal plateGrowth cartilage at long bone endsFuses ~18–25 yrsGH/IGF-1 during developmentArticular cartilageJoint surface; not bone
Limited repairLow-impact loading + nutrition
Key Cellular Players
Osteoblasts — bone-forming cells that secrete collagen matrix (osteoid) and mineralize it with hydroxyapatite. The primary target of pro-growth stimuli.
Osteoclasts — bone-resorbing cells. Controlled resorption is necessary for remodeling; excess resorption leads to net boneloss.
Osteocytes — mature osteoblasts embedded in bone matrix; act as mechanosensors, signaling osteoblasts when strainthresholds are exceeded (via sclerostin suppression and Wnt pathway activation).
Periosteal cells (cambium layer) — resting progenitors that can differentiate into osteoblasts under mechanical or hormonalstimulus responsible for periosteal (outer diameter) growth.
02 | HORMONAL OPTIMIZATION
exists,this section focuses exclusively on natural methods to optimize anabolic hormonal milieu.

Figure 2 — The hormonal hierarchy governing bone formation, from primary anabolic drivers to modulating and catabolic signals.
The GH→IGF-1 axis is the master anabolic regulator for bone. GH is secreted in pulses, primarily during slow-wave sleep andimmediately after high-intensity exercise. IGF-1, produced in the liver and locally in bone, directly stimulates osteoblastproliferation and survival.
InterventionGH ↑ MechanismMagnitude of EffectPractical ActionDeep Sleep (SWS)Largest GH pulse occursin first 90-min SWS cycle↑↑↑↑↑ (dominant driver)Dark, cool room; 8–9h; no blue light 90min before bedHigh-Intensity ExerciseLactate & acidosis signalhypothalamus GHRH release↑↑↑↑Sprint intervals, heavy lifts, plyometrics; keep sessions <60 minIntermittent FastingLow insulin disinhibitsGH secretion↑↑↑ (2–5× baseline)16:8 or 24h fast; ensure nutrition targets still metCold ExposureNorepinephrine →GHRH stimulation↑↑ (transient)5–10 min cold shower/plunge post-trainingSauna (heat stress)Heat shock proteins& GHRH upregulation↑↑↑ (2–16× baseline)20 min, 80°C sauna, 2–4×/week; hydrate wellL-Arginine (oral)Inhibits somatostatin;GH releasing effect↑↑ (10–30%)5–10g pre-sleep on empty stomach; combine with exerciseAvoid hyperglycemiaInsulin blunts GH pulsefor 2–4h↑↑ (by avoiding suppression)sion) No high-GI carbs within 2h of sleep; limit sugar
Testosterone & Androgens (Natural Optimization)
Testosterone directly stimulates periosteal bone growth and increases cortical bone thickness. Men with higher freetestosterone consistently show greater bone cross-sectional area. DHT (dihydrotestosterone) is particularly potent for periosteal expansion.
• Heavy compound resistance training (3–5×/week) → ↑ testosterone 15–30%
• Optimize zinc and magnesium (both co-factors for testosterone synthesis)
• Maintain body fat 10–20% (adipose converts testosterone to estrogen via aromatase)
• Adequate dietary fat (>0.5g/kg/day) — steroid hormones are cholesterol-derived
• Minimize chronic stress (cortisol directly suppresses LH → ↓ testosterone)• Avoid endocrine disruptors: BPA plastics, phthalates, excess alcohol
Estrogen (Critical for Both Sexes)
Estrogen is the primary brake on bone resorption it suppresses osteoclast activity and extends osteoblast lifespan. Bothmales and females require adequate estrogen for bone maintenance. In men, ~20% of circulating estrogen is critical for bone.During female puberty, estrogen drives rapid longitudinal and periosteal growth but ultimately seals the growth plates.
Every Natural & Superficial Method to Maximize Bone Density, Thickness & Architecture
igure 1 — The five major input pathways that converge to drive net bone growth, and the five structural outcomes they produce.
Bone is a dynamic, metabolically active tissue undergoing constant remodeling. Understanding what can be influenced andwhat cannot is the foundation of any effective protocol
StructureWhat It IsCan It Grow?Primary StimulusPeriosteumFibrous membrane wrapping bone outer surfaceYES outer diameterCompressive/tensile mechanical loadCortical (compact)Dense outer shell; ~80% of bone massYES thicknessHigh-impact loading, androgensTrabecular (cancellous)Inner spongy lattice at epiphysesYES density/architecture Impacttecture Impact + nutrition + hormonesEndosteumInner surface lining medullary cavitYES variableHormonal signaling (PTH, estrogen)Epiphyseal plateGrowth cartilage at long bone endsFuses ~18–25 yrsGH/IGF-1 during developmentArticular cartilageJoint surface; not bone
Limited repairLow-impact loading + nutrition
Key Cellular Players
Osteoblasts — bone-forming cells that secrete collagen matrix (osteoid) and mineralize it with hydroxyapatite. The primary target of pro-growth stimuli.
Osteoclasts — bone-resorbing cells. Controlled resorption is necessary for remodeling; excess resorption leads to net boneloss.
Osteocytes — mature osteoblasts embedded in bone matrix; act as mechanosensors, signaling osteoblasts when strainthresholds are exceeded (via sclerostin suppression and Wnt pathway activation).
Periosteal cells (cambium layer) — resting progenitors that can differentiate into osteoblasts under mechanical or hormonalstimulus responsible for periosteal (outer diameter) growth.
• Osteoclasts resorb old/damaged bone (2–3 weeks)
• Osteoblasts fill the cavity with new osteoid (3–4 months)
• Mineralization of osteoid with Ca/P crystals (weeks–months)
• Net result: if formation > resorption → BONE GAIN; if resorption > formation → BONE LOSS
• Osteoblasts fill the cavity with new osteoid (3–4 months)
• Mineralization of osteoid with Ca/P crystals (weeks–months)
• Net result: if formation > resorption → BONE GAIN; if resorption > formation → BONE LOSS
02 | HORMONAL OPTIMIZATION
exists,this section focuses exclusively on natural methods to optimize anabolic hormonal milieu.
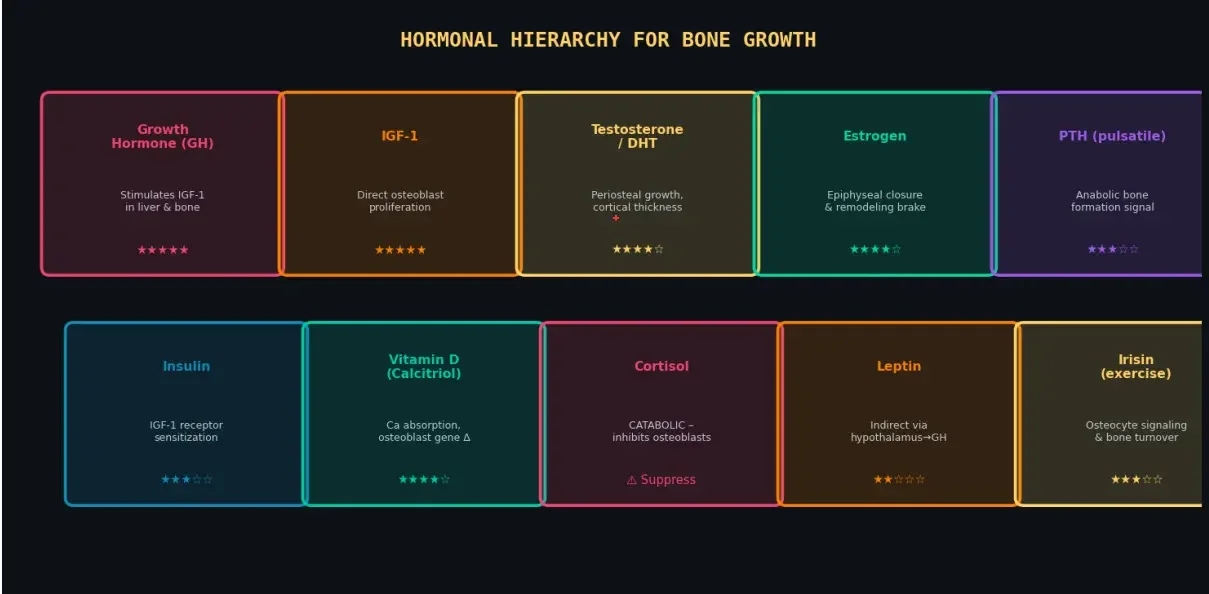
Figure 2 — The hormonal hierarchy governing bone formation, from primary anabolic drivers to modulating and catabolic signals.
The GH→IGF-1 axis is the master anabolic regulator for bone. GH is secreted in pulses, primarily during slow-wave sleep andimmediately after high-intensity exercise. IGF-1, produced in the liver and locally in bone, directly stimulates osteoblastproliferation and survival.
InterventionGH ↑ MechanismMagnitude of EffectPractical ActionDeep Sleep (SWS)Largest GH pulse occursin first 90-min SWS cycle↑↑↑↑↑ (dominant driver)Dark, cool room; 8–9h; no blue light 90min before bedHigh-Intensity ExerciseLactate & acidosis signalhypothalamus GHRH release↑↑↑↑Sprint intervals, heavy lifts, plyometrics; keep sessions <60 minIntermittent FastingLow insulin disinhibitsGH secretion↑↑↑ (2–5× baseline)16:8 or 24h fast; ensure nutrition targets still metCold ExposureNorepinephrine →GHRH stimulation↑↑ (transient)5–10 min cold shower/plunge post-trainingSauna (heat stress)Heat shock proteins& GHRH upregulation↑↑↑ (2–16× baseline)20 min, 80°C sauna, 2–4×/week; hydrate wellL-Arginine (oral)Inhibits somatostatin;GH releasing effect↑↑ (10–30%)5–10g pre-sleep on empty stomach; combine with exerciseAvoid hyperglycemiaInsulin blunts GH pulsefor 2–4h↑↑ (by avoiding suppression)sion) No high-GI carbs within 2h of sleep; limit sugar
Testosterone & Androgens (Natural Optimization)
Testosterone directly stimulates periosteal bone growth and increases cortical bone thickness. Men with higher freetestosterone consistently show greater bone cross-sectional area. DHT (dihydrotestosterone) is particularly potent for periosteal expansion.
• Heavy compound resistance training (3–5×/week) → ↑ testosterone 15–30%
• Optimize zinc and magnesium (both co-factors for testosterone synthesis)
• Maintain body fat 10–20% (adipose converts testosterone to estrogen via aromatase)
• Adequate dietary fat (>0.5g/kg/day) — steroid hormones are cholesterol-derived
• Minimize chronic stress (cortisol directly suppresses LH → ↓ testosterone)• Avoid endocrine disruptors: BPA plastics, phthalates, excess alcohol
Estrogen (Critical for Both Sexes)
Estrogen is the primary brake on bone resorption it suppresses osteoclast activity and extends osteoblast lifespan. Bothmales and females require adequate estrogen for bone maintenance. In men, ~20% of circulating estrogen is critical for bone.During female puberty, estrogen drives rapid longitudinal and periosteal growth but ultimately seals the growth plates.
