





Nodal
its in your blood
- Joined
- Jan 24, 2026
- Posts
- 1,827
- Reputation
- 4,834
This thread is one of the greatest threads made on the Org, I mean it.
It has every single anatomical feature and every single landmark I could find. It includes every single nosemaxxing method, identifying silly copes, and the price of each procedure in different countries. I included citations for every claim I make so you can fact-check yourself.
There is a TL;DR for lazy guys, highlighted text for skimmers, and extreme detail for people who love to read things like this. I even included code for a program that can measure your nose.
I made the formatting quite simple because the Org character limit would not let me post more than 300k characters and I wrote 660k. JFL, but thanks to @DildoFaggins , he helped me lock the thread so I can post the remaining parts in replies. There is so much I could tell you about this thread that I could make another thread about it. It took me 3 weeks of working to get this shit done. So please bump or rep this.
This is possibly my last thread. I might leave the forum, but I am 50/50 right now, so I do not know. Don't take my word for it.
It has every single anatomical feature and every single landmark I could find. It includes every single nosemaxxing method, identifying silly copes, and the price of each procedure in different countries. I included citations for every claim I make so you can fact-check yourself.
There is a TL;DR for lazy guys, highlighted text for skimmers, and extreme detail for people who love to read things like this. I even included code for a program that can measure your nose.
I made the formatting quite simple because the Org character limit would not let me post more than 300k characters and I wrote 660k. JFL, but thanks to @DildoFaggins , he helped me lock the thread so I can post the remaining parts in replies. There is so much I could tell you about this thread that I could make another thread about it. It took me 3 weeks of working to get this shit done. So please bump or rep this.
This is possibly my last thread. I might leave the forum, but I am 50/50 right now, so I do not know. Don't take my word for it.
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
▸ THE MALE NOSE
▸ ANATOMY, IDEALS & FIXES
Understand your anatomy, the ideals, and how to max it
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
NOSE IS LIKE SUPER IMPORTANT
── ME ──
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
▸ QUICK SUMMARY
▸ THE MALE NOSE
▸ ANATOMY, IDEALS & FIXES
Understand your anatomy, the ideals, and how to max it
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
NOSE IS LIKE SUPER IMPORTANT
── ME ──
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
▸ QUICK SUMMARY
Coverage: ANATOMY IDEALS FIXES
Sections: 11 anatomy sections + metrics + ethnic norms + surgical/non-surgical fixes
things i will be covering: 45+ measurements, 30+ anatomical things , 40+ methods for fixing every flaw
probably even more i lost count
▸ TABLE OF CONTENTS
Introduction
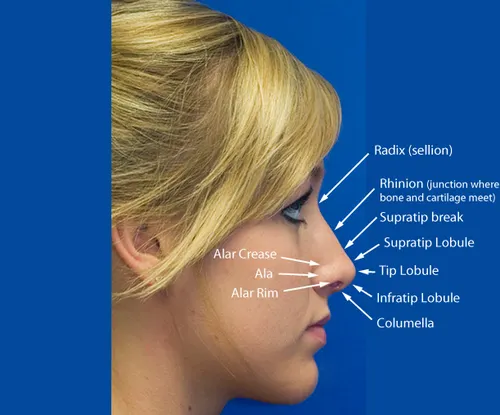
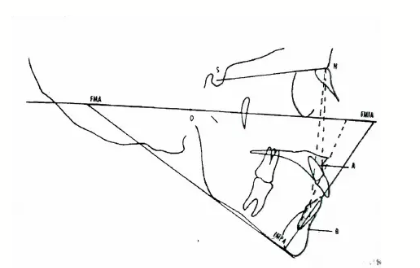
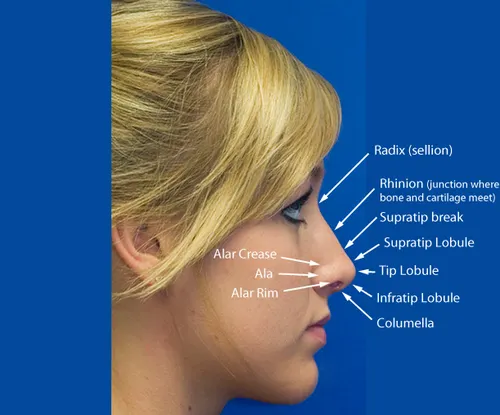
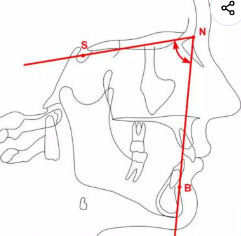
Anatomy of the Nose and Landmarks
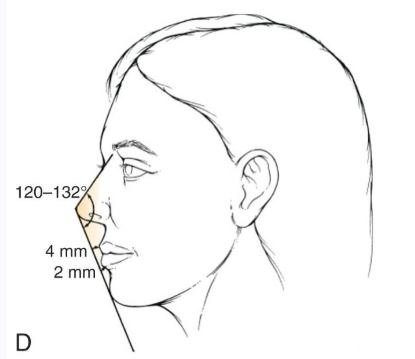
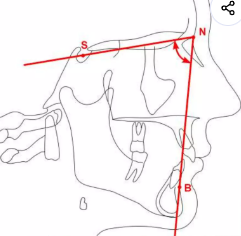
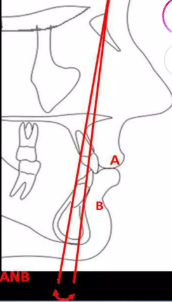
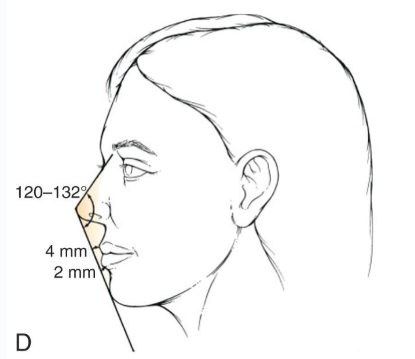
Nasal Metrics, Ethnic Variability, Norms & Ideals
How to Max and Fix Your Nose (Surgical)
Non-Surgical Options & Decision Trees
Choosing a Surgeon & Closing Thoughts
Measure Your Own Nose (DIY Coding)
Research Gaps & Limitations (24 Known Gaps)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
CHAPTER 1
▸ INTRODUCTION
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
You may be desperate, taking pictures from 100 angles to convince your nose is "FINE", trying borderline BS and anything that you come across on your FYP on TikTok.
You are ready to give up, leave all the BS behind, and LDAR. Is there no hope left?
Fuck no. The nose is one of the most studied facial features and researched on. You would be stupid if you gave up on it.
But the nose is one of the most complex and confusing things with a lot of BS information around and myths. So worry not; I will be helping you guys out to know your nose, the ideal, and how to max it.
i have highlited the main points for skimmers
i have made a tldr at the end for lazycels or
you could just look at the flaw fixing part only
For people who want to know as much as possible, let's dive in.
So here we are going to cover:
Anatomy and landmarks
Ideals and norms
How to max and fix your nose
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
CHAPTER 2
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
THIS IS GOING TO BE SUPER LONG
SO I PUT IT IN SPOILERS
DONT TRY TO OPEN EVERYTHING
IF YOU WANT TO READ THE WHOLE THING HERE IS THE TXT FILE
the txt file
Attachments
-
 6409722_1780838081860.png86.3 KB · Views: 0
6409722_1780838081860.png86.3 KB · Views: 0 -
nose_guide_clean.txt285.2 KB · Views: 0
-
 6374595_1780305740316.png196.2 KB · Views: 0
6374595_1780305740316.png196.2 KB · Views: 0 -
 6374731_1780308815212.png7.7 KB · Views: 0
6374731_1780308815212.png7.7 KB · Views: 0 -
 6398753_1780679425460.png56.5 KB · Views: 0
6398753_1780679425460.png56.5 KB · Views: 0 -
 6403861_1780749397266.png45.7 KB · Views: 0
6403861_1780749397266.png45.7 KB · Views: 0 -
 6403899_1780749960116.png44.8 KB · Views: 0
6403899_1780749960116.png44.8 KB · Views: 0 -
 6403919_1780750248011.png43.2 KB · Views: 0
6403919_1780750248011.png43.2 KB · Views: 0 -
 6404003_1780751247022.png42.2 KB · Views: 0
6404003_1780751247022.png42.2 KB · Views: 0 -
 6404003_1780751247022 (1).png42.2 KB · Views: 0
6404003_1780751247022 (1).png42.2 KB · Views: 0 -
 6404085_1780752009192.png36.1 KB · Views: 0
6404085_1780752009192.png36.1 KB · Views: 0 -
 6409612_1780836077638.png50 KB · Views: 0
6409612_1780836077638.png50 KB · Views: 0









 (you understand?
(you understand?










