fushisushi
Iron
- Joined
- Jul 12, 2025
- Posts
- 20
- Reputation
- 29
Today I'm gonna review the best ways of getting BONE GROWTH (with pictures)
(don't forget to like)
I splitted it into paragraphs (from most to least IMPORTANT), hope you like it, provided with sources down below.
pls like the post


6 — daily rhythm, and meal timing
(don't forget to like)
I splitted it into paragraphs (from most to least IMPORTANT), hope you like it, provided with sources down below.
pls like the post
1: Quick summary (what actually increases bone growth)
- Bone length and peak bone mass are driven by genetics plus modifiable factors: nutrition (adequate calories, protein, calcium, vitamin D and other micronutrients), mechanical loading (weight-bearing and impact exercise, resistance training), and endocrine environment (GH → IGF-1 axis, sex steroids). Lifestyle (sleep, stress, smoking, medication exposure) strongly modifies how these factors work.
By the way, this thing is all you need in puberty and we gonna talk about it:

2 — Basic physiology you need to understand
- Bone growth (longitudinal length) happens at the growth plates (epiphyseal plates) during puberty; bone mass (density/size) increases via bone modeling/remodeling in response to mechanical load and hormones. Peak bone mass is mostly accrued during adolescence and early adulthood; building a higher peak bone mass reduces long-term fracture risk. So don't stress over it as a 13-15 year old teenager.
- Growth hormone (GH) is secreted in pulses (big pulse during slow-wave sleep and after intense exercise). GH stimulates the liver to produce IGF-1 (Insulin-like growth factor 1), which is the main effector on bone growth and osteoblastic activity. IGF-1 production is modulated by nutrient signals (notably insulin and amino acids). PubMed+1
- Insulin is anabolic for liver IGF-1 production (insulin increases GH receptor expression and hepatic IGF-1 output), but chronically high insulin (from excess added sugars/ultra-processed diets) has counterproductive metabolic effects. Fructose is processed mainly in the liver and is less insulinogenic than glucose but can cause adverse hepatic effects if consumed in excess. MDPI+1
3 — Hormones and pharmacology (what helps vs what harms)
- Help bone growth / peak bone mass: physiological GH pulses (sleep and exercise), IGF-1 (requires GH + nutrient/insulin signals), sex steroids (estrogen/testosterone during puberty — they both accelerate bone accrual), thyroid hormone at normal levels. OUP Academic
- Sleep: Get to bed early, recommended time ~22:00 but not later than 01:00, get at least 8 hours of sleep, 70% of GH produces in first hours of your sleep, make sure conditions are perfect, 18-23 degrees temperature, fresh air, dark room, no blue light exposure 1h before the bed, don't take naps (will be harder to sleep at night)

- Harm bone growth / peak bone mass: (avoid this shit at ALL COST) chronic glucocorticoid exposure (steroids), cigarette smoking, excessive alcohol, severe under-nutrition, untreated endocrine disorders (hypothyroidism, GH deficiency), some anticonvulsants or other long-term drugs — these can reduce bone accrual or damage growth plates. See a pediatrician if you take regular medication.
4 — Nutrition: exact targets and practical advice
Principles: meet calorie needs for growth, distribute protein across meals, meet calcium and vitamin D, get adequate magnesium/zinc/vitamin K through diet, and avoid chronic excess added sugars (especially concentrated fructose sources like sugary drinks).- Energy and protein
- Don’t restrict calories while you’re growing — energy availability drives growth and hormone balance. Aim to eat enough to support daily activity and growth. PMC
- Adolescent protein targets (practical): typical RDAs translate to roughly ~46 g/day for 14–18 y females and ~52 g/day for 14–18 y males, or roughly 0.8–1.5 g/kg/day depending on activity and growth phase. For athletes or heavy training, higher intakes near 1.3–1.9 g/kg/day may be useful in practice; distribute protein across meals (20–30 g per meal is a simple target). CHOC - Children's Health Hub+1
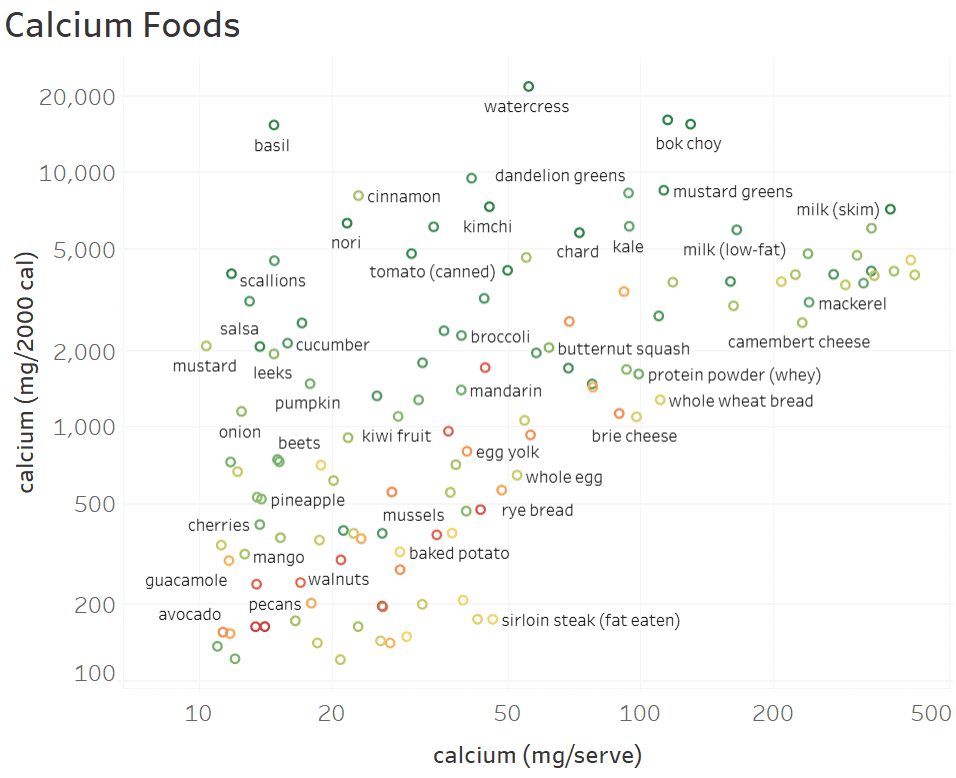
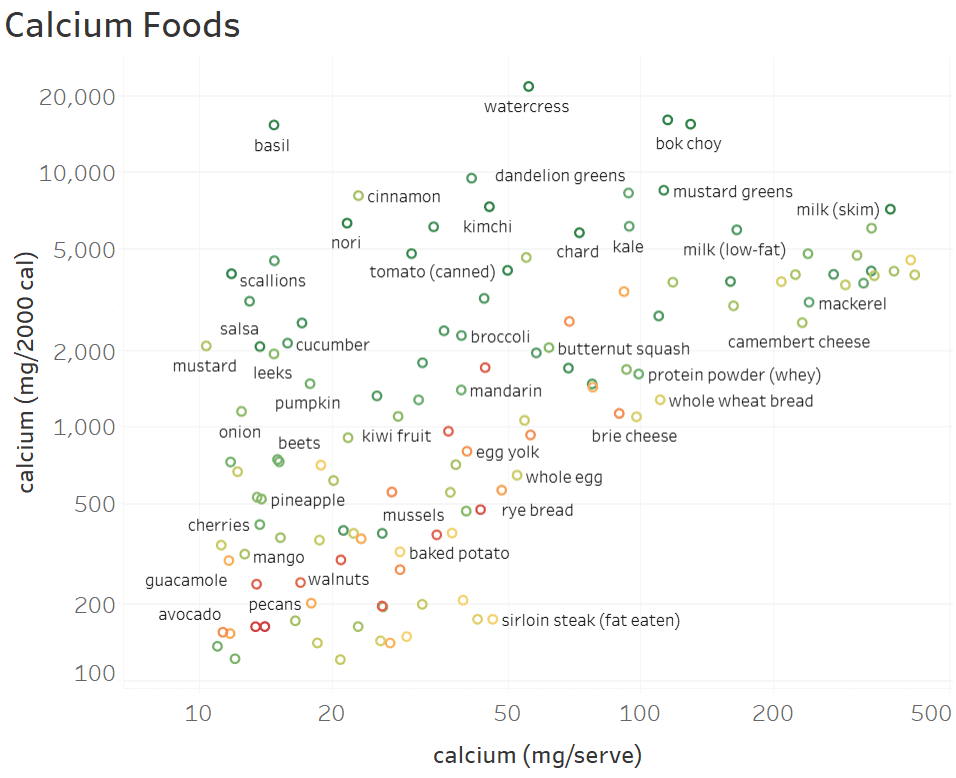
- Calcium
- Adolescents (9–18 y): recommended intake ≈ 1,300 mg/day. Prioritize dairy (milk, yogurt, cheese), calcium-fortified foods, leafy greens and calcium-rich fish. If your diet is poor in calcium, speak with a pediatrician about supplements rather than guessing.
I recommend low-fat milk (abt 402 mg of calcium per cup) as an additional calcium source


- Adolescents (9–18 y): recommended intake ≈ 1,300 mg/day. Prioritize dairy (milk, yogurt, cheese), calcium-fortified foods, leafy greens and calcium-rich fish. If your diet is poor in calcium, speak with a pediatrician about supplements rather than guessing.
- Vitamin D
- RDA ~ 600 IU/day (15 µg) for teens; vitamin D is required for calcium absorption. If you’re indoors a lot or in low sun seasons, a doctor can check serum 25-OH vitamin D and recommend supplementation if required.
Supplementation with calcium and vitamin D is goated.
- RDA ~ 600 IU/day (15 µg) for teens; vitamin D is required for calcium absorption. If you’re indoors a lot or in low sun seasons, a doctor can check serum 25-OH vitamin D and recommend supplementation if required.
- Magnesium, zinc, vitamin K (K2)
- These micronutrients support bone matrix formation, osteoblast function, and osteocalcin activity. Eat nuts, seeds, whole grains, legumes, leafy greens, and animal/fermented foods (for K2). Routine high-dose supplementation is not necessary unless a deficiency is shown. PMC Science Direct
- These micronutrients support bone matrix formation, osteoblast function, and osteocalcin activity. Eat nuts, seeds, whole grains, legumes, leafy greens, and animal/fermented foods (for K2). Routine high-dose supplementation is not necessary unless a deficiency is shown. PMC Science Direct
- Carbohydrates & fructose
- Glucose/starch (rice, oats, potatoes, whole grains) generate a stronger insulin response than pure fructose and therefore support the insulin signal that helps hepatic IGF-1 production when paired with GH and protein. That makes starchy carbs useful in post-exercise meals to assist IGF-1/action. MDPI
- Fructose is a monosaccharide that is primarily metabolized in the liver and is less insulinogenic per gram than glucose; chronic high isolated fructose (sodas, HFCS) can promote fatty liver and metabolic dysfunction and is not a good strategy for healthy bone/hormone status. Whole fruit is fine because fiber/food matrix moderates the load.
5 — Exercise prescriptions that maximize bone accrual
Mechanical load is one of the strongest stimuli for bone modeling in youth.- Key principles: bones adapt to unusual, rapidly applied loads. High-impact, odd-direction, and resistance loads are most osteogenic. Source
An example of simple trainings for those who can't afford gym or other type of activities: - Practical weekly plan (safe, evidence-based):
- Resistance (strength) training: 2–3 sessions/week, focusing on multi-joint movements (squats, deadlifts variations, lunges, push/pull) with progressive overload appropriate for your age and supervision. Resistance training improves muscle and bone strength.
- High-impact/plyometric (jumping) work: 2 sessions/week, 40–100 jumps per session (evidence shows 40–100 jumps, cumulatively, performed consistently over months improves bone mass in adolescents). Start lower and progress; ensure proper landing mechanics and adequate strength first.
- Weight-bearing aerobic activity: walking, running, soccer, basketball — include regularly (3–5 days/week). Non-osteogenic sports (cycling, swimming) should be complemented by impact/resistance training if your goal is bone accrual.
- Safety: do progressive overload slowly, warm up, and train under coach/teacher supervision to avoid joint injuries. If you have existing joint pain, medical clearance is necessary.
6 — daily rhythm, and meal timing
Meal timing for hormonal synergy
To maximize the GH → IGF-1 pathway without suppressing GH pulses: avoid large, high-glycemic meals immediately before main sleep (to preserve nocturnal GH). Use a post-workout window to take starchy carbs + protein (e.g., rice + chicken, oats + milk) so insulin and amino acids support hepatic IGF-1 while GH from exercise and recovery is elevated. MDPI
7 — Orthodontics / retainers — effect on growth
Many of y'all asked how retainers affect forward growth:- Retainers do not stop skeletal growth. If you only had braces and retainers (no palatal expander), the retainer holds teeth in place; it does not “hold” maxillary skeletal expansion because that requires a palatal expansion procedure. Retainers will not prevent natural forward or downward growth of the maxilla/mandible. If you had a palatal expander previously, retention is required after expansion until bone stabilizes. (This is orthodontic, not endocrine.)
8 — What to avoid (common pitfalls)
- Chronic low-calorie dieting, repeated energy deficits, very low protein diets — these suppress IGF-1 and blunt bone accrual. PMC
- Smoking, heavy alcohol, anabolic androgenic steroid misuse, chronic prescription glucocorticoids (unless medically necessary) — all harm bone modeling and should be avoided. ncbi gov
- Excessive added sugars / sugary drinks, especially high in isolated fructose (HFCS), because of detrimental liver/metabolic effects; fruit in whole form is acceptable. ncbi gov
9 — Monitoring, tests, and when to seek medical input
- Routine monitoring is clinical (height tracking, growth charts) and by an orthodontist/pediatrician. If you or your parents are concerned about your growth rate, delayed puberty, or prior medical therapy (e.g., steroid use), see a pediatrician or pediatric endocrinologist. They can measure growth velocity, bone age, and order labs (IGF-1, thyroid function, sex steroids) or imaging (DXA) if indicated. DXA interpretation in adolescents requires pediatric expertise (Z-scores, not T-scores). PMC
10 — A realistic, safe daily plan for a 12-16 year old (example)
- Sleep: 9–10 h nightly (fixed bedtime/wake time). PubMed
- Training: 3 sessions/week — 2 resistance sessions (~30–45 min) + 2 short plyometric sessions (start 30–50 jumps/session) on nonconsecutive days. Add sports (soccer/basketball) or brisk running 2–3×/week. PMC+1
- Nutrition: three balanced meals + 1–2 snacks: each main meal with ~20–35 g protein (eggs, dairy, meat, legumes), starchy carbohydrate (rice/oats/potato), and vegetables. Aim for calcium-rich foods to reach ~1,300 mg/day; vitamin D 600 IU/day from diet or supplements if advised by doctor. Keep added sugar low; prefer whole fruit to fruit juice. Офис диетических добавок+1
- Lifestyle: no smoking, limit alcohol (don’t drink), manage stress (mindfulness/exercise), stay consistent with retainer use if instructed by your orthodontist.
11 — Supplements — cautious notes
- Multivitamin / vitamin D: reasonable if diet or sun exposure is low — have a doctor check blood 25-OH vitamin D first. nih gov
- Calcium supplements: only if dietary intake is insufficient and under pediatric guidance (don’t exceed recommended total). osteoporosis.foundation
- Avoid hormone therapy, prescription GH, or performance steroids unless prescribed and monitored by an endocrinologist — these have real risks and are not appropriate for normal adolescent growth.
I would recommend getting NOW / 21st century Calcium & Magnesium with Vitamin D3 and Zinc supplement, cheap and effective
Sources:
- https://www.ncbi.nlm.nih.gov/books/NBK45503/ — “Determinants of Bone Health” Национальный Центр Биотехники
- https://pubmed.ncbi.nlm.nih.gov/30446875/ — “The effect of a high-impact jumping intervention on bone mass …” PubMed
- https://www.ncbi.nlm.nih.gov/books/NBK45503/figure/ch6.f7/ — figure showing jumping improves hip/lumbar bone mass Национальный Центр Биотехники+1
- https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-015-1633-5 — PRO-BONE study protocol (adolescents + exercise & bone) BioMed Central
- https://pmc.ncbi.nlm.nih.gov/articles/PMC4954586/ — “Genetics of pediatric bone strength” PMC
- https://www.researchgate.net/publication/329018882_The_effect_of_a_high-impact_jumping_intervention_on_bone_mass_bone_stiffness_and_fitness_parameters_in_adolescent_athletes — full-text jumping intervention study ResearchGate
- https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0238127 — “Determinants of bone health in adults Polish women” (supports lifestyle / nutrition effects) PLOS
- https://bjsm.bmj.com/content/52/4/254 — “Positive effects on bone mineralisation and muscular fitness … PRO-BONE results” British Journal of Sports Medicine
- https://www.sciencedirect.com/science/article/abs/pii/S144024401731023X — jump & bone mass in adolescents Научный мир
- https://biomedpharmajournal.org/vol16no3/bone-mineral-density-and-its-determinants-a-systematic-review-of-risk-factors-and-prevention-strategies/ — review on BMD determinants biomedpharmajournal.org
- https://journals.humankinetics.com/view/journals/ijsnem/34/1/article-p38.xml — “Jumping Exercise Combined With Collagen Supplementation Preserves Bone Mineral Density” journals.humankinetics.com