moltisantichincel
2r2c
- Joined
- Jul 2, 2025
- Posts
- 322
- Reputation
- 336
with placing implants comes a risk of masseter dehiscence which just fucks things up. the rate seems to vary between studies with some saying its as high as 20% while others saying its about 2% which makes me wonder if the material and method of placement has to do anything with it.
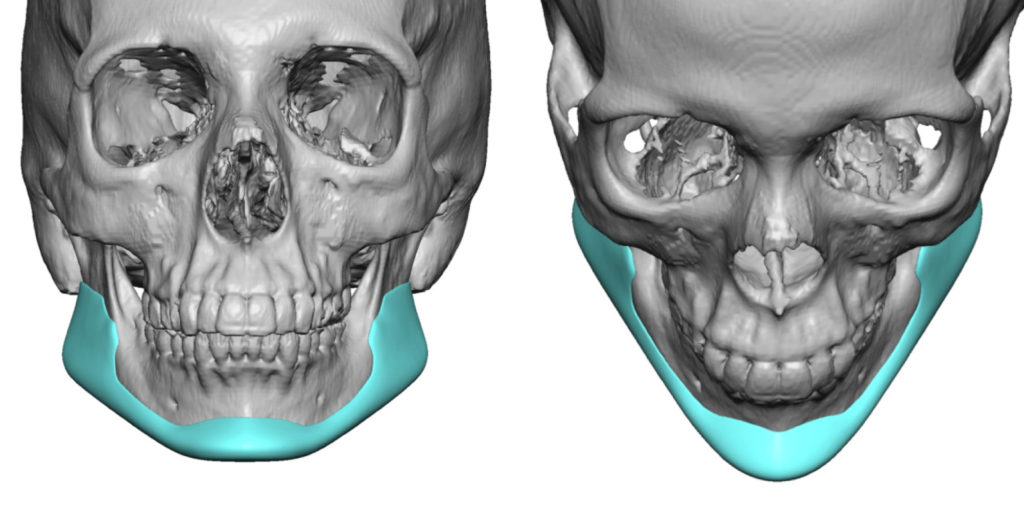
I notice that majority of jaw implants placed are likely silicon with little planning compared to ones that are scrwed (titanium and peek) and the silicone ones always look retarded, I don't know if its the ill informed retarded patients that just think bigger jaw = better which then puts too much preassure on the masseter, which makes sense because if you look at wrap around jaw implants which are always silicone they tend to flare the gonions too much and overall look retarded. (look at the image posted)
Could also be due to the amount of surgical planning, like I said before majority of jaw implants seem to be silicone with less planning than peek or titanium due to them having to be screwed and usually 3d planned. I read this one article from ramieri about his "implate" technique (large titanium bsso plate that also acts as augmentation of the gonions and ramus) and from his 7 patients none of them needed revision or experienced any dehiscence, despite analysis showing a mean mandibular width increase of 18.1 ± 6.2 mm and vertical ramus height gains of 6.0 ± 3.1 mm which is decently significant and is sure to put preassure on the massater, it was only 7 patients tho.
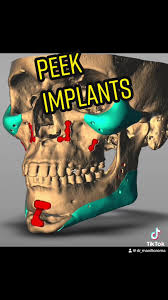
I myself will be getting ramieris mcw implate technique by late 2026 and am worried shits going to go bad, does it covering more of the mandible than his old implate that had a step off increase the risk of dehiscence or does it not matter since the added volume doesn't center around the masseter? (his mcw technique will likely resemble the second image posted except it being a bsso plate and titanium)
But what does everybody else think? is it because of silicone implants, or surgical planning or jewish surgeons, or all of them combined?
@RealSurgerymax from what you have seen which one is the most likely and what do you personally do to mitigate the risk of dehiscence
I notice that majority of jaw implants placed are likely silicon with little planning compared to ones that are scrwed (titanium and peek) and the silicone ones always look retarded, I don't know if its the ill informed retarded patients that just think bigger jaw = better which then puts too much preassure on the masseter, which makes sense because if you look at wrap around jaw implants which are always silicone they tend to flare the gonions too much and overall look retarded. (look at the image posted)
Could also be due to the amount of surgical planning, like I said before majority of jaw implants seem to be silicone with less planning than peek or titanium due to them having to be screwed and usually 3d planned. I read this one article from ramieri about his "implate" technique (large titanium bsso plate that also acts as augmentation of the gonions and ramus) and from his 7 patients none of them needed revision or experienced any dehiscence, despite analysis showing a mean mandibular width increase of 18.1 ± 6.2 mm and vertical ramus height gains of 6.0 ± 3.1 mm which is decently significant and is sure to put preassure on the massater, it was only 7 patients tho.
I myself will be getting ramieris mcw implate technique by late 2026 and am worried shits going to go bad, does it covering more of the mandible than his old implate that had a step off increase the risk of dehiscence or does it not matter since the added volume doesn't center around the masseter? (his mcw technique will likely resemble the second image posted except it being a bsso plate and titanium)
But what does everybody else think? is it because of silicone implants, or surgical planning or jewish surgeons, or all of them combined?
@RealSurgerymax from what you have seen which one is the most likely and what do you personally do to mitigate the risk of dehiscence