TITLE: [GOD-TIER] The Definitive Manifesto on Facial Bone Remodeling & Maxillary Expansion (Puberty/Young Adult Edition)
Preface:
Most of you are playing a losing game. You’re "mewing" with a loose tongue and wondering why your face still looks like a melted candle. If you are in puberty, you are in the only window where you can actually manipulate your skeletal architecture before the sutures fuse. Once you're an oldcel, you aren't "maximizing"; you're just repairing. This guide is for those who want to force a phenotypic shift.
Disclaimer:
This is high-risk, experimental biology. I am not a doctor. Hardmaxxing—specifically peptide use and surgical intervention—carries risks of acromegaly, insulin resistance, and permanent nerve death. DYOR or accept your fate as a mutated thumb.
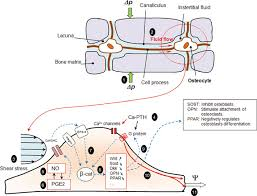
1. Mechanotransduction: This is the process where your cells convert mechanical pressure into chemical signals. When you apply load (chewing/tongue pressure), you activate Piezo1 ion channels in the osteocytes. This triggers a cascade that suppresses Sclerostin (the "stop" signal for bone growth).

2. The Wnt/ββ
-catenin Pathway: When Sclerostin is inhibited, the Wnt pathway is unlocked. This signals osteoblasts to lay down new bone matrix.

1. High-Intensity Mastication (The Mandibular Hammer):

3. Sleep Posture & Gravity Optimization:
1. MK-677 (Ibutamoren):
1. The Peptide Pulse Synergy:
Preface:
Most of you are playing a losing game. You’re "mewing" with a loose tongue and wondering why your face still looks like a melted candle. If you are in puberty, you are in the only window where you can actually manipulate your skeletal architecture before the sutures fuse. Once you're an oldcel, you aren't "maximizing"; you're just repairing. This guide is for those who want to force a phenotypic shift.
Disclaimer:
This is high-risk, experimental biology. I am not a doctor. Hardmaxxing—specifically peptide use and surgical intervention—carries risks of acromegaly, insulin resistance, and permanent nerve death. DYOR or accept your fate as a mutated thumb.
THE THEORY: MECHANOTRANSDUCTION & THE WNT PATHWAY
Before you touch a supplement, understand how bone actually grows. Bone is not a static rock; it is a dynamic tissue.1. Mechanotransduction: This is the process where your cells convert mechanical pressure into chemical signals. When you apply load (chewing/tongue pressure), you activate Piezo1 ion channels in the osteocytes. This triggers a cascade that suppresses Sclerostin (the "stop" signal for bone growth).
2. The Wnt/ββ
-catenin Pathway: When Sclerostin is inhibited, the Wnt pathway is unlocked. This signals osteoblasts to lay down new bone matrix.
- The Secret: Mechanical load + systemic GH/IGF-1 = Hypertrophic Bone Growth. If you have the chemicals (MK-677) without the load (Chewing/Mewing), you just get systemic bloating. If you have the load without the chemicals, the growth is slow and marginal. You need both for the "God-Tier" shift.
METHOD 1: THE MECHANICAL BASELINE (The "Low-Risk" Foundation)
Targeting the Piezo1 channels and skeletal alignment.1. High-Intensity Mastication (The Mandibular Hammer):
- The Tool: Falim or Mastic Gum (Hardness:
≥≥
10/10).
- The Protocol: 60 mins daily, split into two 30-min sessions.
- The Mechanism: Intense loading of the masseter muscles creates periosteal stress on the mandible, forcing the jaw to widen and the chin to project.
- Warning: If you feel a "click" in your TMJ, stop immediately. A recessed jaw is better than a locked jaw.
- The Protocol: Full palatal seal. The entire tongue, including the posterior third (the back), must be pressed against the soft palate.
- The Goal: Constant upward and forward pressure on the maxilla to prevent vertical growth (long face syndrome) and encourage forward projection.
- Nasal Dominance: Mouth breathing is a biological failure. Tape your mouth at night if you have to.
3. Sleep Posture & Gravity Optimization:
- The Protocol: Absolute back-sleeping.
- The Logic: Side-sleeping creates asymmetric compressive forces on the maxilla and mandible, leading to facial asymmetry. Back-sleeping allows for a neutral, non-compressed skeletal state.
- D3 (10k IU) + K2 MK-7 (200mcg): Essential for calcium transport.
- Magnesium (400mg): Required for bone mineralization.
- Collagen (20g) + Vit C: Provides the structural scaffold (Type I Collagen) for the new bone to anchor to.
METHOD 2: THE CHEMICAL CATALYST (The "Mid-Tier" Stack)
Hacking the endocrine system to maximize the response to mechanotransduction.1. MK-677 (Ibutamoren):
- Goal: Mimic ghrelin to spike GH and IGF-1 levels.
- Protocol: 12.5mg - 25mg before bed.
- Cycle: 5 days on / 2 days off.
- Critical: Track your fasting blood glucose. If you hit pre-diabetic levels, you'll get "moon face" edema, which hides the bone growth you're trying to achieve.
- Goal: Dermal-bone remodeling.
- Protocol: 2mg subQ daily.
- Effect: Ensures the skin tightens and conforms to the new, wider bone structure, preventing "loose skin" during growth spurts.
- Goal: Prevent premature epiphyseal closure (closing the growth plates).
- Protocol: Aromasin 12.5mg every other day. Estrogen is what ultimately "locks" your bones; keeping it low during puberty extends the growth window.
METHOD 3: THE NUCLEAR OPTION (The "God" Stack)
For those who are genetically bankrupt and need a total systemic override.1. The Peptide Pulse Synergy:
- CJC-1295 (No DAC) + GHRP-2: 100mcg each, 3x daily on an empty stomach.
- Baseline: MK-677 25mg daily.
- The Logic: CJC/GHRP create massive, acute "pulses" of GH, while MK-677 maintains a high baseline of IGF-1. This is the fastest way to increase bone mineral density and length.
- SAM-e (1500mg) + MSM (1000mg): Based on the hypothesis that maintaining DNA methylation levels prevents the premature closure of the mid-palatal suture and growth plates.
- MSE (Maxillary Skeletal Expansion): The only way to widen a narrow palate post-puberty. It uses a screw to physically split the suture.
- BSSO (Bilateral Sagittal Split Osteotomy): Surgical advancement of the mandible. The final solution for severe recession.
- Zygomatic Implants: Adding width to the cheekbones if the orbital support is insufficient.
SUMMARY EXECUTION TABLE
| Tier | Focus | Primary Agent | Mechanism | Risk Level |
| Foundation | Mechanotransduction | Hard Chewing/Mewing | ↓↓ Sclerostin →→ ↑↑ Wnt | Low (TMJ) |
| Chemical | Endocrine Spike | MK-677 / Aromasin | ↑↑ IGF-1 / ↓↓ Estrogen | Medium (Glucose) |
| Nuclear | Systemic Overhaul | CJC-1295 / MSE | Max GH Pulse / Skeletal Split | High (Surgery/Hormonal) |