MK 6-7
Iron
- Joined
- Jul 20, 2025
- Posts
- 64
- Reputation
- 25
Hello people of knowledge.
I have been looking for a shortcut in my Physical Body development.
Currently i am a skinny 17.5 year old, 190cm, 66kg, 10% bodyfat. I do only have like 1 Month experience, you may call me lazy and stupid for not atleast training 1 year and maybe i am. But i just can‘t be skinny anymore, when i go outside with a T-Shirt on, and feel like people are looking (which they probably arent, it makes me depressed).
So i have decided to take SARMs due to not being able to inject Peptides or Roids, cuz i still live with my parents and have no chance in explaining or getting away with it.
I have informed myself about RAD140, LGD-4033 and LGD-3033 but now i need your help to learn from your experiences, i am looking at doing an 8 week cycle with either one of these SARMs, adding Mk-667 (20mg) + Enclomiphene (12.5mg during cycle) + proper PCT.
Eating and training plan: Upper/Lower, 3500kcal 250g Protein.
What i dont wanna risk is longterm infertility, thats my only worry, i have everything else to protect my cholesterine and Liver.
I am looking to gain 10kg within 3 months, mostly lean muscle so i dont loose all gains after cycle. What do yall think is the best for muscle gain, which is best for fertility safety, and which is best overall. Any advices for or against Sarms im ready to hear.
Thanks for taking your time reading allat.
(Before mk hate comes in i need it for appetite due to me getting full fast).
I have been looking for a shortcut in my Physical Body development.
Currently i am a skinny 17.5 year old, 190cm, 66kg, 10% bodyfat. I do only have like 1 Month experience, you may call me lazy and stupid for not atleast training 1 year and maybe i am. But i just can‘t be skinny anymore, when i go outside with a T-Shirt on, and feel like people are looking (which they probably arent, it makes me depressed).
So i have decided to take SARMs due to not being able to inject Peptides or Roids, cuz i still live with my parents and have no chance in explaining or getting away with it.
I have informed myself about RAD140, LGD-4033 and LGD-3033 but now i need your help to learn from your experiences, i am looking at doing an 8 week cycle with either one of these SARMs, adding Mk-667 (20mg) + Enclomiphene (12.5mg during cycle) + proper PCT.
Eating and training plan: Upper/Lower, 3500kcal 250g Protein.
What i dont wanna risk is longterm infertility, thats my only worry, i have everything else to protect my cholesterine and Liver.
I am looking to gain 10kg within 3 months, mostly lean muscle so i dont loose all gains after cycle. What do yall think is the best for muscle gain, which is best for fertility safety, and which is best overall. Any advices for or against Sarms im ready to hear.
Thanks for taking your time reading allat.
(Before mk hate comes in i need it for appetite due to me getting full fast).



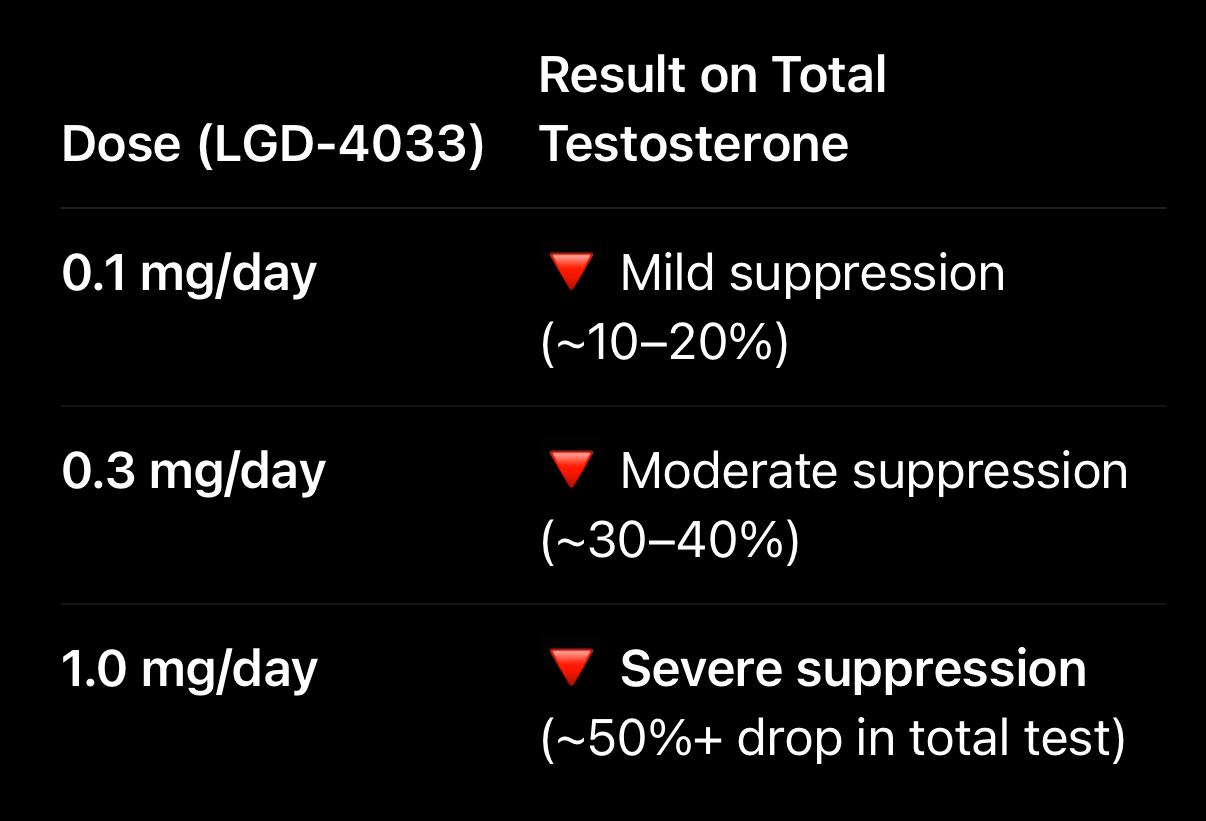
 a study in lgd has shown that males had 0.1mg lgd-4033 for 21 days and their LH got suppressed severely.
a study in lgd has shown that males had 0.1mg lgd-4033 for 21 days and their LH got suppressed severely.