C
crimson297
Iron
- Joined
- Dec 7, 2021
- Posts
- 6
- Reputation
- 7
Long-time lurker, first-time poster.
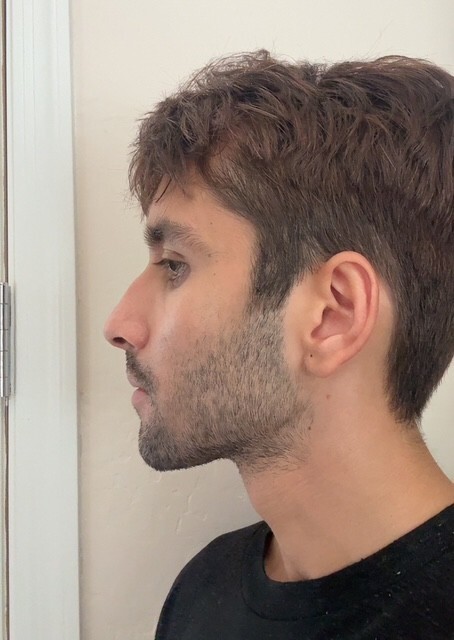
I believe that my most pressing flaws and accompanying fixes are as follows, but I would really appreciate any insight as far as the order to do said procedures and if I have them ranked by ROI appropriately.
1. Periorbital fat grafting
Both upper and lower-eye. I currently have extensive UEE exposure and discoloration + deep tear troughs, which really helps me to Tung Tung Tung Sahurmaxx. However, I notice that when I squint like an idiot it looks substantially healthier. After seeing some great fat-grafting results on the site I am wondering if this alone would be enough to fix my eye area and if this is the #1 ROI procedure for me?
2. Rhinoplasty
Dorsal hump and excessive nasal flare, I think it looks alright from the front and 3/4 angle, but my side profile is poor.
3. Sliding Genioplasty
I believe I have some chin retrusion going on, though I feel like this may be lower priority.
Do I have the right idea? Any other alternative procedures you would suggest? Would I need implants to achieve the eye-area I am going for or would the fat-grafting alone be sufficient?
Of course, I am still working on soft-maxxes as well by getting leaner with Retatrutide, MT-1 to tan, will re-perm (Asian salon botched it jfl), neck training + improve posture, etc.
I believe that my most pressing flaws and accompanying fixes are as follows, but I would really appreciate any insight as far as the order to do said procedures and if I have them ranked by ROI appropriately.
1. Periorbital fat grafting
Both upper and lower-eye. I currently have extensive UEE exposure and discoloration + deep tear troughs, which really helps me to Tung Tung Tung Sahurmaxx. However, I notice that when I squint like an idiot it looks substantially healthier. After seeing some great fat-grafting results on the site I am wondering if this alone would be enough to fix my eye area and if this is the #1 ROI procedure for me?
2. Rhinoplasty
Dorsal hump and excessive nasal flare, I think it looks alright from the front and 3/4 angle, but my side profile is poor.
3. Sliding Genioplasty
I believe I have some chin retrusion going on, though I feel like this may be lower priority.
Do I have the right idea? Any other alternative procedures you would suggest? Would I need implants to achieve the eye-area I am going for or would the fat-grafting alone be sufficient?
Of course, I am still working on soft-maxxes as well by getting leaner with Retatrutide, MT-1 to tan, will re-perm (Asian salon botched it jfl), neck training + improve posture, etc.