





Pyridostigmine is an acetylcholinesterase inhibition, meaning it prevents the breakdown of acetylcholine (ACh), leading to a build up of ACh, leading to enhanced cholinergic signalling at muscarinic and nicotinic receptors.
Pyridostigmine does NOT cross the blood brain barrier, so the increased ACh does not impact cognition, however due to the fact the regions of the hypothalamus involved in endocrinal control lay outside the BBB, pyrostigamine can influence hypothalamic endocrinal signalling.
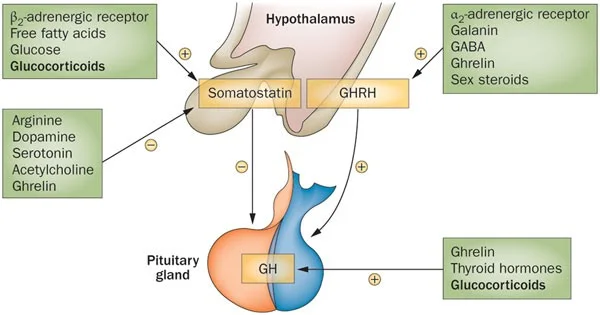
GH secretion from the pituitary is governed by a dual hypothalamic mechanism:
GHRH (Growth Hormone Releasing Hormone): Stimulates GH synthesis and release
Somatostatin: Inhibits GH release by blocking the intracellular cAMP and Ca2+ pathways initiated by GHRH

For a GH pulse to occur, there must be a simultaneous increase in GHRH and a decrease in somatostatin.
When pyridostigmine leads to a build up of ACh in the hypothalamus, the binding of ACh to muscaniric ACh receptors on somatostatinergic neurons causes the the release of somatostatin to be inhibited.
By suppression somatostatin, pyrostigmine removes the inhibitory blocker of GH release, this means the hypothalamus becomes hypersensitive to endogenous GHRH release, so more GH is released per GHRH pulse.

However, pyridostigmine is most powerful when combined with an exogenous GHRH, like CJC-1295.

Unfortunately tachyphylaxis (tolerance) can occur extremely quickly

Due to this, I theorise pyridostigmine should be used in a cycled manner.
I have been doing 2 days on, 2 days off, however I will arrange a number blood tests (soon) to find the most optimal usage pattern.
There are pros and cons of using either the IR or XR version of pyrostigamine:
Pyri has a short half-life, so somatostatin would only be inhibited for a few hours, using XR means a higher basal level of GH all round rather than just single supraphysiological pulses
However having constant inhibition of somatostatin could accelerate tachyphylaxis, causing faster downregulation
Therefore it may be more beneficial to just time pyro dosing with GHRH injections and sleep
I am currently using IR
In one study, cholinergic side effects occured in 30% of participants, including:
Mild Abdominal Pain
Amdominal Cramps
Muscle twitching
I have not experienced any side effects so far
This is an entirely experimental therapy, i believe i am the first person to ever do this therapy off label for gh, im still experimenting to find the best way to conduct it, or whether this is even a viable therapy considering the tachyphylaxis, however heres what i have noticed so far:
Immediately noticable effects using as a monotherapy:
Better sleep (I dose right before bed)
Less muscle fatigue the day after training
Waking earlier
When using as a tri-therapy with CJC-1295 and ipamorelin, i lower the dosage of CJC-1295, I essentially get all of the same effects just greater, i have not used pyro long enough to give an extensive anecdote
Pyridostigmine does NOT cross the blood brain barrier, so the increased ACh does not impact cognition, however due to the fact the regions of the hypothalamus involved in endocrinal control lay outside the BBB, pyrostigamine can influence hypothalamic endocrinal signalling.
GH secretion from the pituitary is governed by a dual hypothalamic mechanism:
GHRH (Growth Hormone Releasing Hormone): Stimulates GH synthesis and release
Somatostatin: Inhibits GH release by blocking the intracellular cAMP and Ca2+ pathways initiated by GHRH
For a GH pulse to occur, there must be a simultaneous increase in GHRH and a decrease in somatostatin.
When pyridostigmine leads to a build up of ACh in the hypothalamus, the binding of ACh to muscaniric ACh receptors on somatostatinergic neurons causes the the release of somatostatin to be inhibited.
By suppression somatostatin, pyrostigmine removes the inhibitory blocker of GH release, this means the hypothalamus becomes hypersensitive to endogenous GHRH release, so more GH is released per GHRH pulse.
SO YEAH IT INCREASES GH NIGGA

However, pyridostigmine is most powerful when combined with an exogenous GHRH, like CJC-1295.
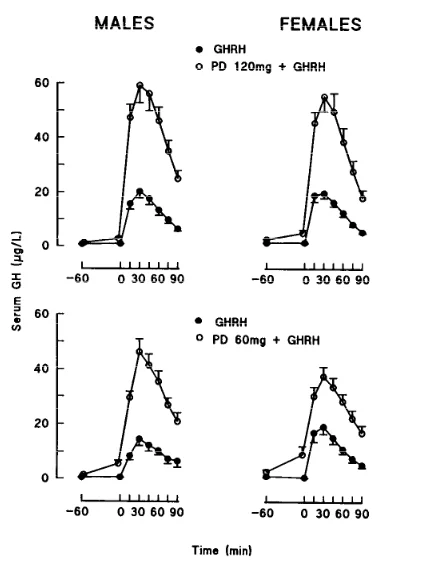
A 300% INCREASE
(This is likely the same to how it would impact endogenous GHRH, just relative)So how should we use it????
Cycling
Unfortunately tachyphylaxis (tolerance) can occur extremely quickly

Due to this, I theorise pyridostigmine should be used in a cycled manner.
I have been doing 2 days on, 2 days off, however I will arrange a number blood tests (soon) to find the most optimal usage pattern.
Instant Release vs Extended Release
There are pros and cons of using either the IR or XR version of pyrostigamine:
Pyri has a short half-life, so somatostatin would only be inhibited for a few hours, using XR means a higher basal level of GH all round rather than just single supraphysiological pulses
However having constant inhibition of somatostatin could accelerate tachyphylaxis, causing faster downregulation
Therefore it may be more beneficial to just time pyro dosing with GHRH injections and sleep
I am currently using IR
Side effects
In one study, cholinergic side effects occured in 30% of participants, including:
Mild Abdominal Pain
Amdominal Cramps
Muscle twitching
I have not experienced any side effects so far
This is an entirely experimental therapy, i believe i am the first person to ever do this therapy off label for gh, im still experimenting to find the best way to conduct it, or whether this is even a viable therapy considering the tachyphylaxis, however heres what i have noticed so far:
Immediately noticable effects using as a monotherapy:
Better sleep (I dose right before bed)
Less muscle fatigue the day after training
Waking earlier
When using as a tri-therapy with CJC-1295 and ipamorelin, i lower the dosage of CJC-1295, I essentially get all of the same effects just greater, i have not used pyro long enough to give an extensive anecdote