strong_silent_type
Lefort 3 is the answer
- Joined
- Dec 14, 2019
- Posts
- 658
- Reputation
- 704

The standard osteotomy used for distraction osteogenesis of the hypoplastic maxilla is LeFort I. An advancement of more than 10 mm in patients with no cleft and 6 mm in patients with CLP is beyond the limit of LeFort I osteotomy, and in such cases distraction osteogenesis for advancement of the maxilla can be used. Distraction osteogenesis (DO) is a biological process involving the formation of new bone between viable bone segments that are gradually separated by incremental traction.
[...]
The gradual increase in soft tissue volume in response to the tension forces applied with bony distraction is called “distraction histogenesis”. Conventional LeFort I osteotomy provides immediate bone advancement but, however, does not allow for compensatory growth of the soft tissues. The high rate of relapse after conventional maxillary advancement seems to be a result of scarring and memory of the soft tissues, though the soft tissue often contracts to its pre-operative state. On the other hand, DO creates a gradual increase in the amount of soft tissue by preventing its contraction [21].
[...]
High-level complete LeFort I osteotomy is the most commonly performed osteotomy since tooth buds are located on a standard level of LeFort I osteotomy line in young patients [1, 36, 39–43]. Standard LeFort I and the 3-piece LeFort I osteotomies are also used with this protocol [7, 26, 35, 44, 45].
[...]
Sagittal distraction forces produce not only advancement forces at the intermaxillary sutures but also higher stress values at the sutura nasomaxillaris, sutura frontonasalis and sutura zygomaticomaxillaris on the cleft side of the patients with unilateral cleft lip and palate rather than the non-cleft side. Some patients feel pressure under the eyes, around the lateral nasal walls and generally throughout the face during and after the distractor activations.
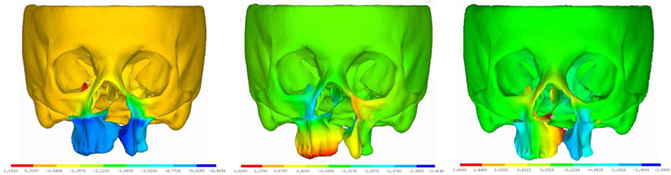
Figure 6.
Displacement distribution in (a) sagittal, (b) transversal and (c) vertical planes after 6 mm of maxillary advancement for the UCLP model, respectively.
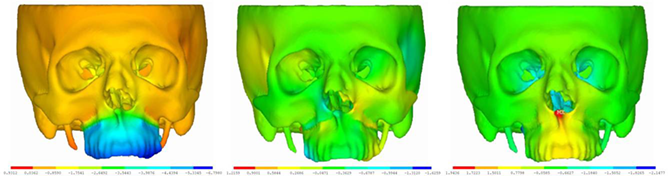
Figure 7.
Displacement distribution in (a) sagittal, (b) transversal and (c) vertical planes after 6 mm of maxillary advancement for the non-cleft control model, respectively.
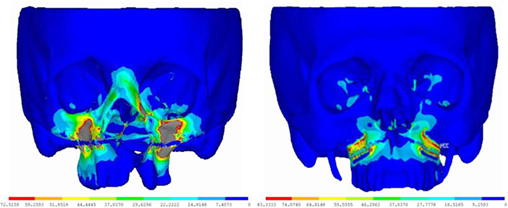
Figure 8.
The magnitude and distribution of the von Mises stresses after 1 mm of maxillary advancement for the UCLP model and for the non-cleft control model, respectively.
[...]
The application of the force according to the center of resistance of the maxilla plays an important role in sagittal maxillary advancement. The mostly desired directions of the maxillary movements in DO are forward and downward. The center of the mass of the maxilla is considered to be located at the apex of the maxillary premolars. When the force is applied at the center of resistance of the maxilla, a straight anterior movement of the maxilla without any rotation is expected. If the same force is applied above, a clockwise rotation will be expected with a predictable increase in over bite and overjet negligible mandibular rotation. If the force is applied below, a counterclockwise rotation will be expected with a tendency of an anterior open bite
Distraction Osteogenesis in the Treatment of Maxillary Hypoplasia
The aim of this chapter is to review literature reporting on the use of internal distraction osteogenesis and rigid external distraction osteogenesis and to determine the biomechanical effects of internal distractors in the treatment of maxillary hypoplasia, especially in patients with cleft lip...
 www.intechopen.com
www.intechopen.com

Attachments

Last edited: