

RealSurgerymax

From .net
- Joined
- Jul 24, 2020
- Posts
- 3,485
- Reputation
- 11,680
Hello Everyone,
In the last year Shoulder Widening has become a big topic on the forums and last week Leif Rogers published a new procedure on YouTube, although I haven't seen anything in the journals yet.
Shoulder Reduction Surgery for the MtF Plastic Surgery population has shown us that clavicle length can be modified which has a direct effect on shoulder width with good predicatble outcomes, with reasonable recovery, as a low-risk outpatient procedure.
Almost all Elective Aesthetic Surgeries are derived from the reconstructive. Shoulder widening surgery was first performed on children with congenitally short clavicles which affected form and function to an extent corrective surgery was warranted. In one case, the surgeon used a Distraction Osteogenesis and in the other, Iliac (hip) Bone Grafts to widen their clavicles.
Now, aesthetic shoulder widening, on an elective basis has come about. You have a few options: Iliac Crest Graft, Fibula Graft, Sliding Clavicle Osteotomy, Distraction Osteogeneis, and Alloplastic Interpositional Bone Implant (PEEK, Theoretical). I will explain them for you below:
Interpositional Bone Graft Option 1 - Iliac (Hip) Harvest
This is the osteotomy used by pediatric reconstructive surgery but could be used in an adult as well. The Iliac Crest is a common bone harvest site for Plastic and Maxillofacial Surgeries and leaves a scar on the side of your hip.
Two small (3cm) skin incisions at the bottom of your neck are made and your clavicles are divided with a saw. The blocks of bone cut from the crest of the hip are inserted between the divided ends of the collar bone, essentially lengthening it, plated with special clavicle plates and closed. The bone graft is integrated into the new clavicle and the edges smooth over the course of about a year when plates can be removed if desired.
The downside to this procedure is the scar and possible irregularity left at the hip harvest site - although if performed bilaterally under a modified technique could be viewed as a good thing for those who desire fip narrowing (although this effect would be minimal if at all noticeable, and certainly limited as the lower hip remains just as wide.)
As with any free bone graft there are risks of infection and loss of the graft.
 Maximum Widening: About 2cm Bilaterally, limited by the harvest site.
Maximum Widening: About 2cm Bilaterally, limited by the harvest site.
Other Effects: Shoulders Roll Backward (Aesthetically Viewed positively)
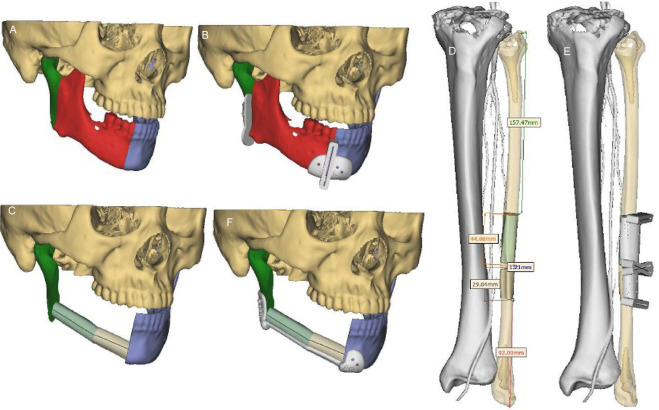
Interpositional Bone Graft Option 2 - Fibula (Lower Leg) Harvest
This is one of the the versions proposed by Dr Eppley as a modification of the above procedure. He talks about it in many places on his blog and and Q&A.
The lower leg has 2 bones, the Tibia and the Fibula. Plastic and Maxillofacial Surgeons commonly harvest the fibula to reconstruct a new mandible (for those who unfortunately lost their lower jaw to cancer or trauma to a rarer extent.) The Tibia supports about 85% of the load placed on it, so loss of the fibula can be adjusted to very well, particularly by young, healthy and highly motivated people. Many of these Jaw Reconstruction patients are substance abusers, in poor health and of more advanced age than most people here who are mostly ASA Class I. Further the surgery to the harvest site would be much less extensive than in the mandibular reconstruction version since less bone is needed, and also that the mandibular reconstruction also removed an entire paddle of skin and muscle.
As above, this is another bone graft. The small risk of infection and possible bone loss necessitating reoperation still applies. It is superior in that the graft site provides the possibility for more lengthening. Being a long bone, the limitation is set by literally how much the shoulder can be widened without injuring the related muscles, ligaments and nerves and that is about 2.5cm bilaterally, possibly up to 3cm in some people.
 Maximum Widening: About 2.5cm Bilaterally, limited by the related soft tissues ability to strecth without injury.
Maximum Widening: About 2.5cm Bilaterally, limited by the related soft tissues ability to strecth without injury.
Other Effects: Shoulders Roll Backward (Aesthetically Viewed positively)
Interpositional Bone Graft Option 3 - Allogenic (Cadaver Bone)
This option is similar to the methods described above, exceot instead of using your own bone (Autologous) it uses a block cadaver bone matrix which your own bone will grow into and across.
It may be a more inferior option to an autologous graft. Much has been written about Autologous Bone Grafts (Rib, Iliac, Fibula, Calvarial) vs. Allogenic Bone. Which is better depends on the application. Unfortunately when it comes to clavicle lengthening, we just don't know yet.
 Maximum Widening: About 2.5cm Bilaterally (Possibly with more resorption), limited by the related soft tissues ability to strecth without injury.
Maximum Widening: About 2.5cm Bilaterally (Possibly with more resorption), limited by the related soft tissues ability to strecth without injury.
Other Effects: Shoulders Roll Backward (Aesthetically Viewed positively)
Sliding Clavicle Osteotomy
Most Recently, Leif Rogers published a YouTube video performing his method of Clavicle Lengthening. Think of it as a BSSO of the Clavicle. The Osteotomy is made at a slant and it is slid on itself to lengthen the shoulders. When I first heard about this, my concern was that the bone will be too thin where the two divided sides are left in contact. While they do seem thin to me, not necessarily unacceptably so, and he places some Allogenic Bone Putty (allogenic bone discussed above) over the osteotomy for the bone to grow into as it heals.
The advantages of this method is reduced risk of bone graft infection and bone loss (if the putty got infected it would not jeopardize the result as much as an interpositional bone graft becoming infected) as well as no need for a harvest site (no scar or recovery involved at the hip or lower leg.
The only disadvantage is a smaller amount of widening, 1.5 to 2cm. This is still an adequate and noticeable improvement. Here is the video:
Maximum Widening: About 1.75cm Bilaterally, limited by the the need for enogh bone to be in contact on both sides of the sliding osteotomy
Other Effects: Shoulders Roll Backward (Aesthetically Viewed positively)
Distraction Osteogenesis
This is another technique which has been used before in the reconstructive world. The advantage is the Distraction Histogensis (Soft Tissue Stretching and Regeneration including nerves) which occurs with the Distraction Osteogeneis (Bone Regeneration between the osteotomy.)
The downsides are higher complication, longer recovery and the tendency for the clavicles to roll forward which gives a sad or beaten look/stance. This could potentially be mitigated with a Lengthening-Over-Nail approach which is used in Leg Lengthening sometimes. Intermedulary nails of the clavicle can be technically challenging to place though and now crosses the realm into Orthopedic Surgery and not Plastic Surgery.
Here is an external Long bone Distractor (Depicts a femur but this method was applied to the clavicles)
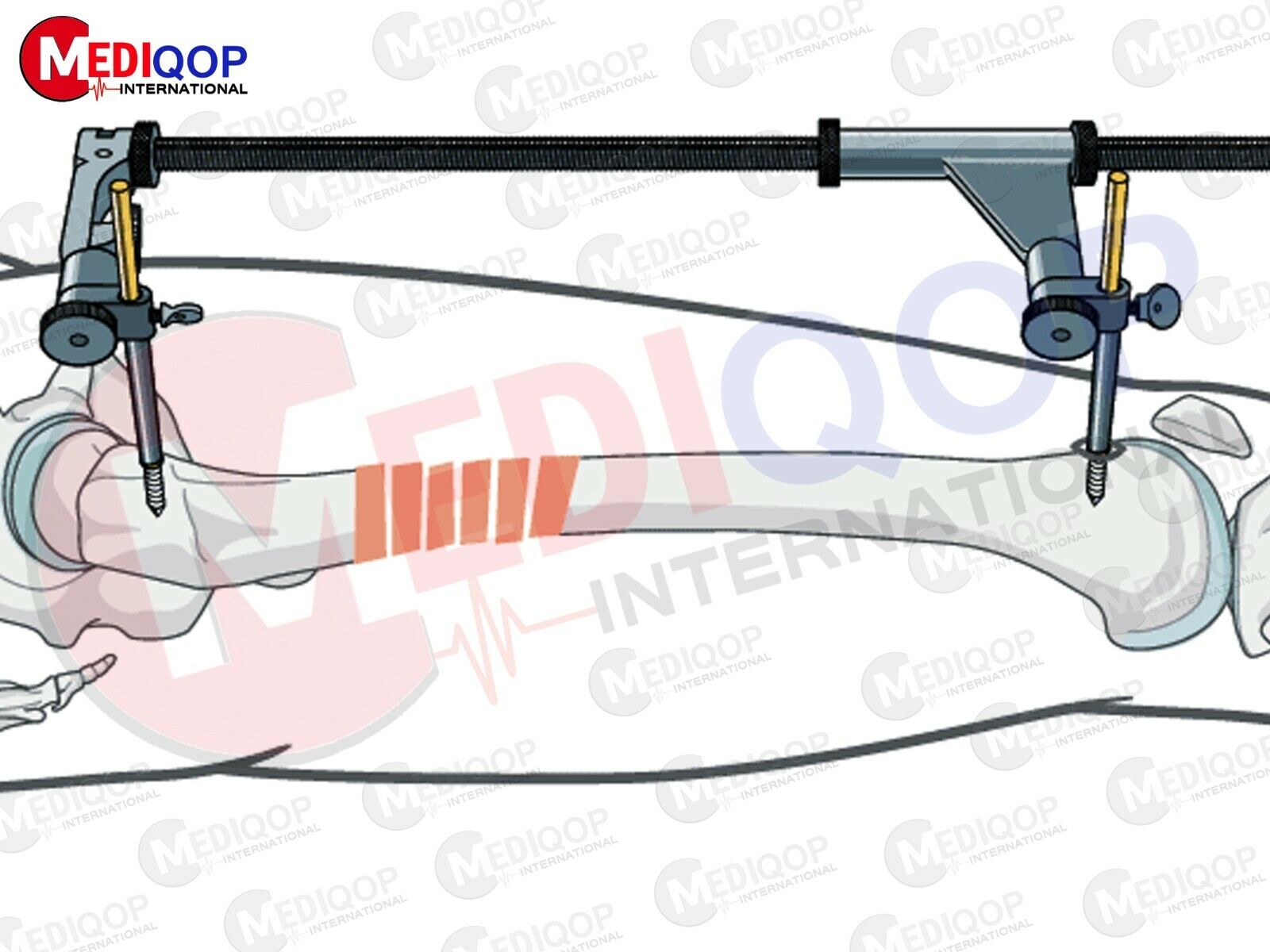 Maximum Widening: 3.5cm or more
Maximum Widening: 3.5cm or more
Other Effects: Shoulders Roll Forward (Aestheticly Viewed Negatively)
Interpositional Alloplastic Implant (Theoretical and not recommended)
Many people might be wondering now if you could just use some non-living material to lengthen the clavicle. The answer is technically yes, if you had to, but it would not be preferred. Even if it worked well after the recovery it could cause problems later in life as bones get weaker.
For shits and giggles there are two similar applications used in Spinal Surgery and by Plastic Surgeons in Chest Wall Reconstructions.
Porous PEEK Implants are used in Vertebral Implants which allow bone ingrowth and work well. Further, entire rib cages including the sternum have been replaced with 3d Printed PEEK:

In the last year Shoulder Widening has become a big topic on the forums and last week Leif Rogers published a new procedure on YouTube, although I haven't seen anything in the journals yet.
Shoulder Reduction Surgery for the MtF Plastic Surgery population has shown us that clavicle length can be modified which has a direct effect on shoulder width with good predicatble outcomes, with reasonable recovery, as a low-risk outpatient procedure.
Almost all Elective Aesthetic Surgeries are derived from the reconstructive. Shoulder widening surgery was first performed on children with congenitally short clavicles which affected form and function to an extent corrective surgery was warranted. In one case, the surgeon used a Distraction Osteogenesis and in the other, Iliac (hip) Bone Grafts to widen their clavicles.
Now, aesthetic shoulder widening, on an elective basis has come about. You have a few options: Iliac Crest Graft, Fibula Graft, Sliding Clavicle Osteotomy, Distraction Osteogeneis, and Alloplastic Interpositional Bone Implant (PEEK, Theoretical). I will explain them for you below:
Interpositional Bone Graft Option 1 - Iliac (Hip) Harvest
This is the osteotomy used by pediatric reconstructive surgery but could be used in an adult as well. The Iliac Crest is a common bone harvest site for Plastic and Maxillofacial Surgeries and leaves a scar on the side of your hip.
Two small (3cm) skin incisions at the bottom of your neck are made and your clavicles are divided with a saw. The blocks of bone cut from the crest of the hip are inserted between the divided ends of the collar bone, essentially lengthening it, plated with special clavicle plates and closed. The bone graft is integrated into the new clavicle and the edges smooth over the course of about a year when plates can be removed if desired.
The downside to this procedure is the scar and possible irregularity left at the hip harvest site - although if performed bilaterally under a modified technique could be viewed as a good thing for those who desire fip narrowing (although this effect would be minimal if at all noticeable, and certainly limited as the lower hip remains just as wide.)
As with any free bone graft there are risks of infection and loss of the graft.
Other Effects: Shoulders Roll Backward (Aesthetically Viewed positively)
Interpositional Bone Graft Option 2 - Fibula (Lower Leg) Harvest
This is one of the the versions proposed by Dr Eppley as a modification of the above procedure. He talks about it in many places on his blog and and Q&A.
The lower leg has 2 bones, the Tibia and the Fibula. Plastic and Maxillofacial Surgeons commonly harvest the fibula to reconstruct a new mandible (for those who unfortunately lost their lower jaw to cancer or trauma to a rarer extent.) The Tibia supports about 85% of the load placed on it, so loss of the fibula can be adjusted to very well, particularly by young, healthy and highly motivated people. Many of these Jaw Reconstruction patients are substance abusers, in poor health and of more advanced age than most people here who are mostly ASA Class I. Further the surgery to the harvest site would be much less extensive than in the mandibular reconstruction version since less bone is needed, and also that the mandibular reconstruction also removed an entire paddle of skin and muscle.
As above, this is another bone graft. The small risk of infection and possible bone loss necessitating reoperation still applies. It is superior in that the graft site provides the possibility for more lengthening. Being a long bone, the limitation is set by literally how much the shoulder can be widened without injuring the related muscles, ligaments and nerves and that is about 2.5cm bilaterally, possibly up to 3cm in some people.
Other Effects: Shoulders Roll Backward (Aesthetically Viewed positively)
Interpositional Bone Graft Option 3 - Allogenic (Cadaver Bone)
This option is similar to the methods described above, exceot instead of using your own bone (Autologous) it uses a block cadaver bone matrix which your own bone will grow into and across.
It may be a more inferior option to an autologous graft. Much has been written about Autologous Bone Grafts (Rib, Iliac, Fibula, Calvarial) vs. Allogenic Bone. Which is better depends on the application. Unfortunately when it comes to clavicle lengthening, we just don't know yet.
Other Effects: Shoulders Roll Backward (Aesthetically Viewed positively)
Sliding Clavicle Osteotomy
Most Recently, Leif Rogers published a YouTube video performing his method of Clavicle Lengthening. Think of it as a BSSO of the Clavicle. The Osteotomy is made at a slant and it is slid on itself to lengthen the shoulders. When I first heard about this, my concern was that the bone will be too thin where the two divided sides are left in contact. While they do seem thin to me, not necessarily unacceptably so, and he places some Allogenic Bone Putty (allogenic bone discussed above) over the osteotomy for the bone to grow into as it heals.
The advantages of this method is reduced risk of bone graft infection and bone loss (if the putty got infected it would not jeopardize the result as much as an interpositional bone graft becoming infected) as well as no need for a harvest site (no scar or recovery involved at the hip or lower leg.
The only disadvantage is a smaller amount of widening, 1.5 to 2cm. This is still an adequate and noticeable improvement. Here is the video:
Maximum Widening: About 1.75cm Bilaterally, limited by the the need for enogh bone to be in contact on both sides of the sliding osteotomy
Other Effects: Shoulders Roll Backward (Aesthetically Viewed positively)
Distraction Osteogenesis
This is another technique which has been used before in the reconstructive world. The advantage is the Distraction Histogensis (Soft Tissue Stretching and Regeneration including nerves) which occurs with the Distraction Osteogeneis (Bone Regeneration between the osteotomy.)
The downsides are higher complication, longer recovery and the tendency for the clavicles to roll forward which gives a sad or beaten look/stance. This could potentially be mitigated with a Lengthening-Over-Nail approach which is used in Leg Lengthening sometimes. Intermedulary nails of the clavicle can be technically challenging to place though and now crosses the realm into Orthopedic Surgery and not Plastic Surgery.
Here is an external Long bone Distractor (Depicts a femur but this method was applied to the clavicles)
Other Effects: Shoulders Roll Forward (Aestheticly Viewed Negatively)
Interpositional Alloplastic Implant (Theoretical and not recommended)
Many people might be wondering now if you could just use some non-living material to lengthen the clavicle. The answer is technically yes, if you had to, but it would not be preferred. Even if it worked well after the recovery it could cause problems later in life as bones get weaker.
For shits and giggles there are two similar applications used in Spinal Surgery and by Plastic Surgeons in Chest Wall Reconstructions.
Porous PEEK Implants are used in Vertebral Implants which allow bone ingrowth and work well. Further, entire rib cages including the sternum have been replaced with 3d Printed PEEK:
Last edited:









