Acromegaly_Chad
Offical Surgery Consultant
- Joined
- Apr 16, 2020
- Posts
- 2,186
- Reputation
- 6,077
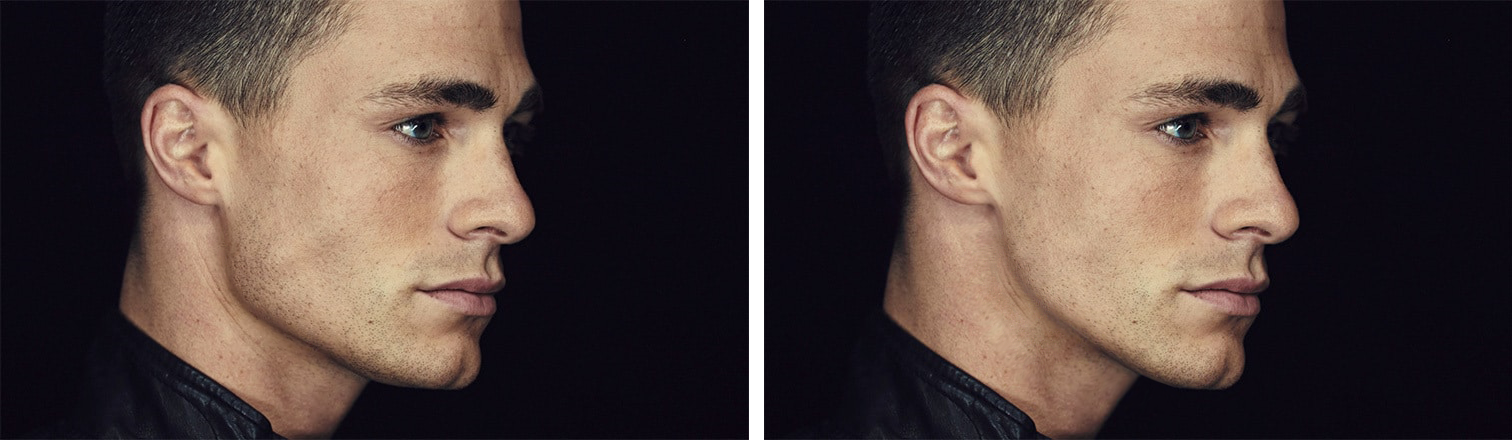
If your gonions are giga inwards tilted just as mine not even a chin wing can safe you. The only option are custom titanium jaw angle implants.
Titanium has been used for decades with very little known complications.
Let's have a look at a study aimed at analyzing compatibility of titanium on your cranium/head to show how well it works:

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
Even further and more detailed information about the usage of jaw angle implants:
Asymmetry and unfavorable esthetics of the jawline have become possible to correct in three dimensions using computer aided design and computer aided manufacturing.

 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
Titanium has been used for decades with very little known complications.
Let's have a look at a study aimed at analyzing compatibility of titanium on your cranium/head to show how well it works:
Object
Decompressive craniectomy is an established procedure to lower intracranial pressure. Therefore, cranioplasty remains a necessity in neurosurgery as well. If the patient's own bone flap is not available, the surgeon can choose between various alloplast grafts. A review of the literature proves that 4–13.8% of polymethylmethacrylate plates and 2.6–10% of hydroxyapatite-based implants require replacement. In this retrospective study of large skull defects, the authors compared computer-assisted design/computer-assisted modeled (CAD/CAM) titanium implants for cranioplasty with other frequently used materials described in literature.Methods
Twenty-six patients underwent cranioplasty with CAD/CAM titanium implants (mean diameter 112 mm). With the aid of visual analog scales, the patients' pain and cosmesis were evaluated 6–12 years (mean 8.1 years) after insertion of the implants.Results
None of the implants had to be removed. Of all patients, 68% declared their outcomes as excellent, 24% as good, 0.8% as fair, and 0% as poor. There was no resulting pain in 84% of the patients, and 88% were satisfied with the cosmetic result, noting > 75 mm on the visual analog scale of cosmesis. All patients would have chosen cranioplasty again, stating an improvement in their quality of life by the calvarial reconstruction. Nevertheless, follow-up images obtained in 4 patients undergoing removal of meningiomas was only suboptimal.Conclusions
With the aid of CAD technology, all currently used alloplastic materials are suited even for large skull defect cranioplasty. Analysis of the authors' data and the literature shows that cranioplasty with CAD/CAM titanium implants provides the lowest rate of complications, reasonable costs, and acceptable postoperative imaging. Polymethylmethacrylate is suited for primary cranioplasty or for long-term follow-up imaging of tumors. Titanium implants seem to be the material of choice for secondary cranioplasty of large skull defects resulting from decompressive craniectomy after trauma or infarction. Expensive HA-based ceramics show no obvious advantage over titanium or PMMA.
Evaluation of clinical outcomes and bone loss around titanium implants with oxidized surface: six-year follow-up results from a prospective case series study - PubMed
Implants with oxidized microtextured surface may achieve excellent long-term clinical outcomes in the rehabilitation of partial edentulism.
pubmed.ncbi.nlm.nih.gov
Even further and more detailed information about the usage of jaw angle implants:
Asymmetry and unfavorable esthetics of the jawline have become possible to correct in three dimensions using computer aided design and computer aided manufacturing.
Aims:
The aim of this study was to provide esthetic, technical, and operative guidelines for mandibular angle and border augmentation using patient-specific titanium implants made by selective laser melting.Settings and Design:
University hospital - prospective registry.Subjects and Methods:
Twelve patients and 17 implantation sites were documented and prospectively registered. Malformational, deformational, and purely esthetic indications were encountered.Statistical Analysis Used:
Descriptive.Results:
Patient satisfaction was high, probably because the patients had input into the planned dimensions and shape. A serious infection with implant removal occurred in one patient who had six previous surgeries at the same sites. Technical and surgical guidelines were developed including splitting implants into two segments when the mental nerve was at risk, using a three-dimensional (3D) puzzle connection, providing at least two screw holes per segment, using scaffolds at the bony contact side, using a “satin” finish at the periosteal side, referring to anatomical structures where possible, making provisions for transbuccal and transoral fixation, using a high vestibular incision, and using a double-layer closure. Esthetic guidelines are discussed but could not be upgraded.Conclusions:
Mirroring techniques and 3D print accuracy up to 0.1 mm allow precise planning of jaw angle implants. Patients are pleased when given preoperative renderings for their consideration. Infections can be managed using technical and operative recommendations and careful patient selection.Guidelines for patient-specific jawline definition with titanium implants in esthetic, deformity, and malformation surgery
Asymmetry and unfavorable esthetics of the jawline have become possible to correct in three dimensions using computer aided design and computer aided manufacturing.The aim of this study was to provide esthetic, technical, and operative guidelines for ...
www.ncbi.nlm.nih.gov